Linking the Malawian Diaspora to the Development of Malawi”
Malawi
Malawi (/məˈlɔːwi,məˈlɑːwi/; Chichewa pronunciation:[maláβi]; Tumbuka: Malaŵi), officially the Republic of Malawi and formerly known as Nyasaland, is a landlocked country in Southeastern Africa. It is bordered by Zambia to the west, Tanzania to the north and northeast, and Mozambique to the east, south and southwest. Malawi spans over 118,484 km2 (45,747 sq mi) and has an estimated population of 19,431,566 (as of January 2021). Malawi’s capital and largest city is Lilongwe. Its second-largest is Blantyre, its third-largest is Mzuzu and its fourth-largest is its former capital, Zomba.
ICT and Communication Ministers from six African countries have confirmed attendance for the Connected Africa Summit 2024.
The six, representing Sierra Leone, Zambia, Namibia, Somalia, Burundi, and Djibouti will join other tech leaders from across the region for the summit happening from the 21st to the 25th of April at Uhuru Gardens in Nairobi.
The event will also have representation from fifteen ambassadors representing African, American, European, Asian and the Middle East.
The ministers are Hon. Salima Monorma Bah (Sierra Leone), H.E. Léocadie Ndacayisaba (Burundi), Hon. Felix Mutati (Zambia), Hon. Mudane Jaamac Xasan Khaliif (Somalia), Hon. Emma Theofelus (Namibia) and Hon. Mr. Radwan Abdillahi Bahdon (Djibouti) with more African ministers also expected to attend the event.
Ambassadors from leading technology and investment markets, including the United States of America Ambassador to Kenya, Margaret “Meg” Whitman, and United Kingdom’s Neil Wigan OBE, are also set to attend the event.
Global and African Ambassadors from the Islamic Republic of Pakistan, Costa Rica, Sierra Leone, Zambia, Malawi, Federal Republic of Somalia, Sahrawi Arab Democratic Republic, Senegal, Burundi, South Africa, South Sudan, Turkey and Zimbabwe have also confirmed their attendance.
The ambassadors are Ms Saqlain Syedah, Pakistan High Commissioner to Kenya, H.E. Mrs. Giovanna Valverde Stark, Ambassador of Costa Rica in Kenya, H.E. Ms. Isatu Aminata Bundu, High Commissioner Permanent Representative to UNON, UNEP & UN HABITAT, H.E. Ms. Joyce Kapamba Kasosa, Zambia High, Commissioner to Kenya, H.E. Mrs. Callista Jennie Mutharika, Malawi High Commissioner to Kenya, H.E. Mr. Jabril Ibrahim Abdulle, Somalia Ambassador to Kenya, H.E. Mr. Mohamed-Liman Ali Ami, Ambassador of the Sahrawi Arab Democratic Republic, (SADR) to Kenya, Amb. H.E. Mr. Ndong Dieng, Ambassador of Senegal to Kenya, H.E. Evelyne Habonimana, Burundi ambassador to Kenya, H.E. Mr. Mninwa Johannes Mahlangu, South African High Commission to Kenya, H.E Mr. Chol Mawud Unguec Ajongo, South Sudanese Ambassador to Kenya, Amb. Subutay Yüksel, Ambassador of Turkey to Kenya, and H.E Winpeg Moyo, Ambassador of Zimbabwe to Kenya.
The summit will focus on Africa’s ICT priorities guided by the African Union’s (AU) Agenda 2063, bringing together African Heads of State, First Ladies, African ICT ministers, policymakers, Global ICT firms, Entrepreneurs, Investors, and Innovators to bridge the digital divide while identifying new investment opportunities.
The Connected Africa Summit 2024 nurtures innovative ideas and partnerships that leverage technology to advance Africa’s development agenda. The Summit is an opportunity for Africa to chart its own path towards the development of its digital economy.
The Summit will act as a platform where African leaders can position the African tech agenda in readiness for the UN Summit of the Future to be held in September 2024 and determine their role in green technology and governance of generative AI for African realities.
Tuberculosis (TB) is a pervasive bacterial infection caused by Mycobacterium tuberculosis (Mtb), contributing significantly to global mortality. Despite Mtb’s latent infection in a substantial proportion of the global population, only a fraction progresses to active TB. The disproportionate burden of TB in Sub-Saharan Africa and Southeast Asia underscores its public health significance.1,2Mycobacterium tuberculosis’s intracellular nature and host-specific interactions highlight the genetic basis of susceptibility.
Numerous studies have explored the connection between genomic loci and TB susceptibility, encompassing candidate genes, family aggregation, twin studies, house contacts, and genome-wide analyses.3 Key players in TB susceptibility include genes encoding proteins such as major histocompatibility complex/human leukocyte antigen (MHC/HLA), tumor necrosis factors (TNFs) and their receptors, immune-related GTPases (IRGs), NRAMP1 (SLC11A1), Toll-like receptors (TLRs), vitamin D nuclear receptor (VDR), and cell surface proteins like collectins.4,5
The complex interplay between host genetics and TB susceptibility underscores the need for a nuanced understanding. While existing literature offers insights, inconsistencies arise, necessitating a deeper exploration of innate immune genes. Genetic polymorphisms associated with TB susceptibility display varying frequencies across populations, suggesting the role of environmental selection pressures.5,6
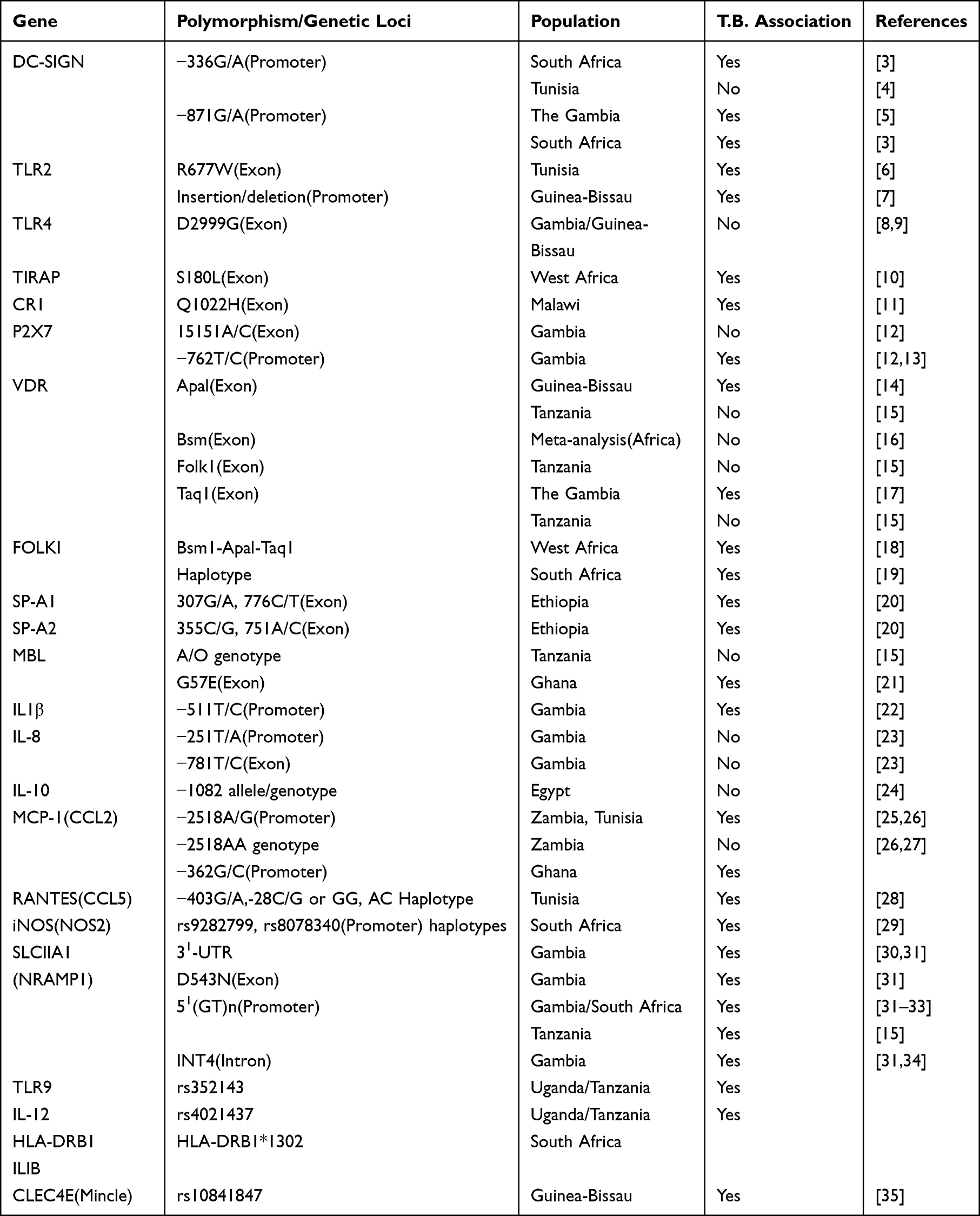
This review focuses on polymorphisms in immune genes linked to pulmonary TB susceptibility in African populations, Table 1. By elucidating the interaction between host molecules and Mtb, we aim to contribute to the design of effective strategies against tuberculosis.
Table 1 Association Studies of Polymorphisms in Immune Genes and Tuberculosis
The African Context
Understanding the genetic basis of tuberculosis (TB) susceptibility is a complex endeavor that requires careful consideration of diverse populations. Focusing on African populations in TB polymorphism studies is a strategic choice driven by various scientific, epidemiological, and ethical considerations. This justification aims to elucidate the rationale behind concentrating exclusively on African populations.
High TB Burden in Africa
Africa bears a substantial burden of TB, with high prevalence rates and a significant impact on public health.7 By concentrating on African populations, we prioritize a region where TB poses a severe threat to community well-being. Tuberculosis in Africa is characterized by a multifaceted interplay of factors, including TB-HIV co-infection, poverty, weak healthcare systems, and drug resistance. These unique challenges underscore the necessity for tailored interventions that address the specific needs of African communities.
Genetic Diversity in African Populations
Africa is characterized by unparalleled genetic diversity, owing to its rich history, diverse ethnicities, and unique population structures.8 Investigating TB polymorphisms in this context allows for a nuanced exploration of genetic variants that may be specific to African populations. This approach aligns with the growing recognition of the importance of population-specific genetic studies.
Prevalence of HIV Co-Infection
TB-HIV co-infection represents a critical aspect of TB epidemiology in Africa. HIV weakens the immune system, heightening susceptibility to TB infection and increasing the risk of TB reactivation among individuals with latent TB. Numerous studies have underscored the strong association between HIV and TB in Africa, with a significant proportion of TB cases occurring among HIV-positive individuals.1,9
Impact of Poverty and Socioeconomic Factors
Poverty and socioeconomic disparities significantly fuel the TB epidemic in Africa. Factors such as poor living conditions, overcrowding, limited healthcare access, and inadequate nutrition contribute to the transmission and persistence of TB in many African communities.10 These challenges exacerbate efforts to control TB and impede the achievement of optimal treatment outcomes.
Challenges Posed by Weak Healthcare Systems
Africa’s healthcare systems grapple with resource constraints, infrastructure deficiencies, and staffing shortages, presenting substantial barriers to effective TB control. Inadequate diagnostic capacities, limited access to quality medications, and suboptimal adherence to treatment regimens further complicate TB management in numerous African countries.11 Strengthening healthcare systems and enhancing access to TB care are paramount for reducing the burden of TB in Africa.
Emergence of Drug Resistance
The emergence of drug-resistant TB strains, including multidrug-resistant (MDR) and extensively drug-resistant (XDR) variants, poses a formidable challenge to TB control efforts across Africa. Limited access to quality diagnostic tools, inappropriate treatment regimens, and poor treatment adherence contribute to the proliferation of drug-resistant TB strains in the region.12 Addressing the menace of drug-resistant TB demands enhanced surveillance, rigorous infection control measures, and expanded access to effective treatment modalities.
Environmental and Socioeconomic Factors
The interplay between genetics and environmental factors is a crucial aspect of TB susceptibility. African populations often face unique environmental challenges and socioeconomic conditions that influence disease dynamics. Investigating TB polymorphisms in this context allows for a holistic understanding of the gene-environment interactions contributing to TB susceptibility.
Precision Medicine and Targeted Interventions
African populations deserve tailored medical interventions that consider their unique genetic makeup. Precision medicine initiatives aim to develop therapies specific to individual genetic profiles.13 By focusing on TB polymorphisms in African populations, we contribute to the development of targeted interventions that address the specific needs of this population. Therefore, the decision to study TB polymorphisms in African populations is rooted in the region’s high TB burden, genetic diversity, unique environmental challenges, and the pursuit of precision medicine. By concentrating our efforts in this context, we aim to unravel population-specific genetic factors influencing TB susceptibility, ultimately contributing to more effective and targeted strategies for TB control in Africa.
Epidemiological Data
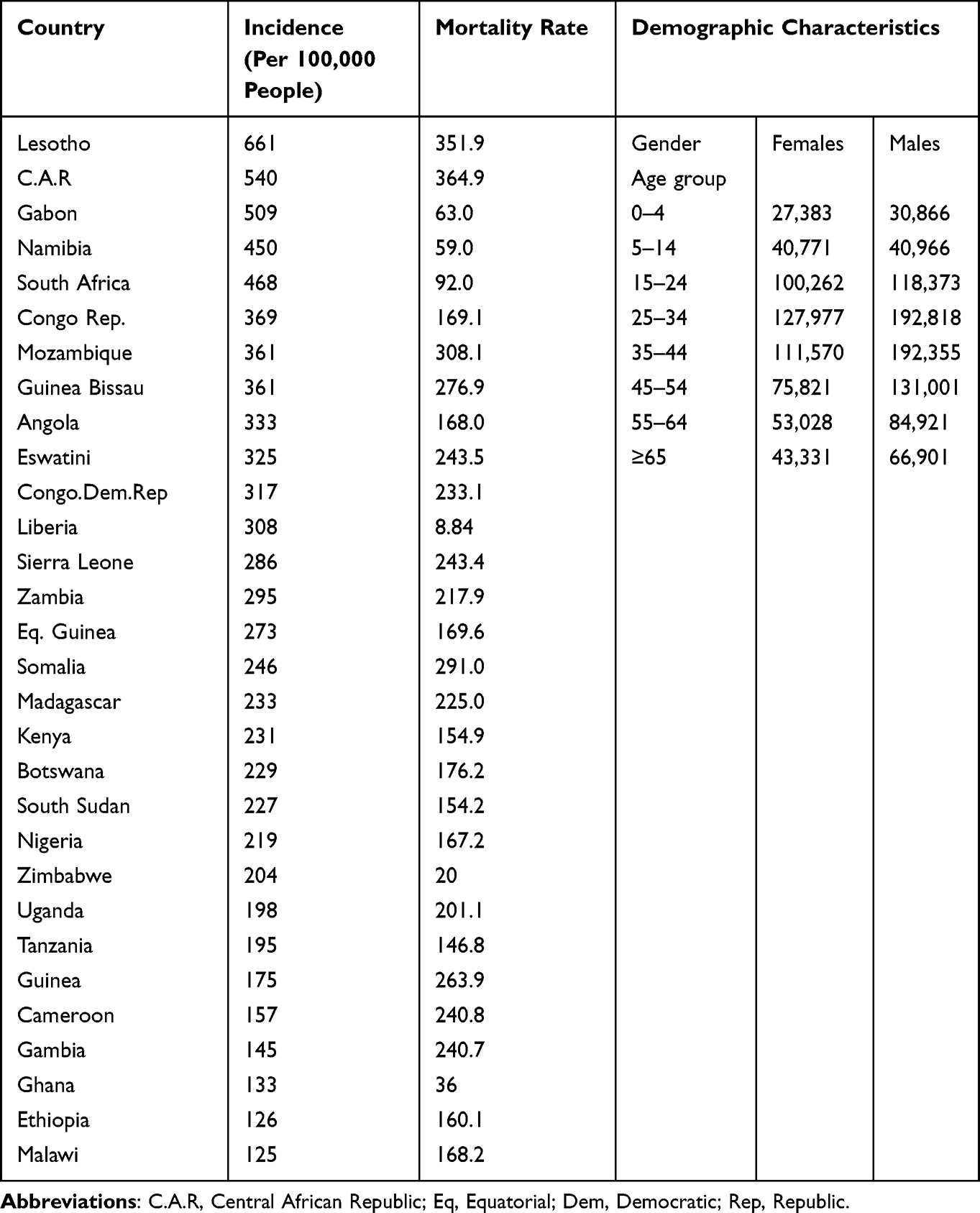
Tuberculosis remains a pressing public health concern, particularly in African populations, where it continues to exert a significant burden on health systems and communities. The incidence rates, mortality rates, and demographic characteristics associated with TB in Africa are shown in Table 2.14
Table 2 The Incidence, Mortality Rates, and Demographic Characteristics Associated with TB in Africa
TB Incidence Rates
Countries such as Lesotho, C.A.R, Gabon, South Africa have the highest Tb incident rates on the continent. However, progress has been made in reducing TB incidence in several African countries through increased access to diagnostic and treatment services, Table 2.
TB Mortality Rates
Somalia, Mozambique, Lesotho and C.A.R are among the countries with the highest TB mortality rates in Africa. TB mortality rates in Africa are closely linked to factors such as HIV co-infection, drug resistance, and healthcare access. While mortality rates have declined in recent years due to improved TB control efforts, they remain significant, particularly in countries with high HIV prevalence.
Demographic Features
Young adults, particularly those in the economically productive age group, are disproportionately affected by TB. Additionally, men are more likely to develop TB than women in many African countries, due to social and behavioral factors as seen in Table 2. Socioeconomic disparities, including poverty, overcrowding, and limited access to healthcare, contribute to the unequal distribution of TB within communities. Urban areas tend to have higher TB burdens due to population density and environmental factors, although rural areas are not exempt from the disease.
Roles of Proteins in Host – Pathogen Interaction
In the realm of tuberculosis susceptibility, extensive research is focused on elucidating the intricate roles of various proteins to decipher the underlying mechanisms governing host-pathogen interaction. These proteins, encompassing Toll-like receptors (TLRs), Dendritic Cell-Specific Intercellular Adhesion Molecule-3 Grabbing Non-Integrin (DC-SIGN), the vitamin D nuclear receptor, soluble C-type lectins such as surfactant proteins A and D, C-type Lectin Domain Family 4 Member E (CLEC4E), and mannose-binding lectin (MBL), represent integral components of the immune system’s response to Mycobacterium tuberculosis (MTB) infection.
As we embark on an in-depth exploration of the nuanced interplay between these proteins and MTB, we intent to uncover their individual and collective contributions to TB susceptibility. Farthermore, discerning the roles of phagocyte cytokines, including Interleukin-1 (IL-1), Interleukin-6 (IL-6), Interleukin-10 (IL-10), Interleukin-12 (IL-12), and Interleukin-18 (IL-18), alongside chemokines such as Interleukin-8 (IL-8), monocyte chemoattractant protein 1 (MCP-1), and Regulated upon activation, normal T-cell expressed and secreted (RANTES). This comprehensive investigation serves to enhance our understanding of the immune response to TB infection, paving the way for novel insights into TB susceptibility mechanisms and potential avenues for therapeutic intervention.
The Human Leukocyte Antigens(HLAs)
The Human Leukocyte Antigen (HLA) molecules are proteins found on the surface of cells in the human body. They play a crucial role in the immune system by presenting antigens, which are fragments of proteins from pathogens like bacteria and viruses, to T cells. This process is essential for the immune system to recognize and respond to foreign invaders while distinguishing them from the body’s own cells. HLA molecules are highly diverse and polymorphic, meaning they exist in many different forms within human populations. This diversity is important for immune system function and contributes to individual differences in immune responses to pathogens, susceptibility to diseases, and compatibility for organ and tissue transplantation.
Recent studies have revealed that specific Human Leukocyte Antigen (HLA) alleles might contribute to either increased or decreased susceptibility to tuberculosis (TB) within African communities.5 For instance, investigations have established correlations between certain HLA class I alleles—such as HLA-B39:01 and HLA-B58:01—and elevated TB susceptibility among West African populations. Conversely, alternative HLA class I alleles, like HLA-B*57:01, have demonstrated a protective association against TB within African cohorts.15,16
Furthermore, HLA class II alleles have emerged as significant factors in TB susceptibility among African populations.16 Notably, research has identified links between particular HLA-DRB1 alleles—such as HLA-DRB115:01 and HLA-DRB104:05—and heightened susceptibility to TB among East and West African groups. Conversely, contrasting HLA-DRB1 alleles, including HLA-DRB110:01 and HLA-DRB111:01, have shown protective effects against TB within African populations.
It is crucial to recognize the intricate nature of the relationship between HLAs and TB susceptibility, influenced by diverse factors such as genetic background, environmental exposures, and host-pathogen interactions. Moreover, the prevalence of specific HLA alleles may exhibit variability across different African populations, underscoring the necessity for population-specific investigations to comprehensively grasp the genetic determinants of TB susceptibility.
Soluble C-Type Lectins (Collectins)
Collectins, including MBL, SP-A, and SP-D, are calcium-dependent lectins crucial for innate immunity. Previous data on calcium-dependent (C type) lectins reveals the close relationship between the bacillus with MBL and SP-A, SP-D17 Specifically, SP-A and SP-D, located in the alveoli and respiratory epithelium, play a pivotal role in the defense against intracellular pathogens, including Mtb. SP-A and SP-D, collagen-like glycoproteins, serve as opsonins, enhancing phagocytosis by alveolar macrophages.17–19 Additionally, SP-A interacts with alveolar macrophages, modulating TLR2 and TLR4 pathways,18 showcasing the intricate immune pathways influenced by these collectins. SP-A’s impact on inflammatory cells depends on the cell state, resulting in the inflammatory paradox. While enhancing cytokine release during infection, SP-A also suppresses macrophage secretion, revealing a complex regulatory role in the immune response.
Polymorphic changes in the genes encoding SP-A and SP-D, particularly in the amino acid sequences, contribute to susceptibility to TB.20 Genetic changes in SP-A and SP-D amino acid sequences have functional consequences. Single nucleotide polymorphisms in these proteins occur when a single nucleotide (adenine, thymine, cytosine, or guanine) in a DNA sequence is altered or substituted with a different single nucleotide at a specific position in the genome. These genetic variants may either result in a synonymous or non-synonymous substitution. Since interactions of SP-A and SP-D with the same and or different pathogens occur. A polymorphism in SP-A reduces binding to Mtb, increasing susceptibility, while a genetic change in SP-D alters the sequence, affecting bacterial surface binding and increasing uptake by alveolar macrophages.
Membrane Binding Lectins (MBL)
Membrane-binding lectin, a soluble pathogen recognition receptor, plays a pivotal role in host defense against bacterial pathogens. Its hexameric structure, akin to the C1q component of the complement system, facilitates the opsonization of microbes, enhancing phagocytosis. MBL also contributes to inflammation by clearing apoptotic cells and releasing cytokines.21,22 MBL gene polymorphisms contribute to variations in blood levels and hexamer formation. MBL gene duplication results in the identification of two genes, MBL1 and MBL2, with MBL2 being the representative in humans. The MBL2 gene encompasses four coding regions (exons) separated by three non-coding regions (introns) at codon positions 52, 54, and 57, featuring variant alleles, D, B, and C, respectively. Certain alleles are linked to impaired hexamer formation and reduced blood levels.5
Mutations at specific codons resulting in low MBL levels increase susceptibility to various infections, particularly in individuals with other immune defects. Despite numerous studies exploring MBL alleles and their polymorphisms (Table 1), inconsistent results underscore the imperative to comprehensively understand the relationship between TB establishment and the polymorphic variants in the MBL gene.
Mannose-binding lectin-2 variants exhibit relatively frequent occurrences, albeit unevenly distributed across human populations.23 Notably, allele B is prevalent in Asian and native South African populations but absent in the West African population. Conversely, allele D is confined to North Africa and Caucasian populations, while allele C is predominant in Sub-Saharan Africa. These allele frequency disparities shed light on the biological advantage of MBL low levels in specific populations.
In summary, individuals with low MBL levels face increased susceptibility to various infections, particularly when coupled with other immune defects. Despite numerous studies exploring MBL alleles and their polymorphisms (Table 1), inconsistent results underscore the imperative to comprehensively understand the relationship between TB establishment and the polymorphic variants in the MBL gene. Notably, the allele frequency disparities observed, especially the prevalence of allele B in certain populations and the restriction of allele D to specific regions, shed light on the biological advantages associated with MBL low levels in distinct populations. Further investigations are warranted to unravel the precise mechanisms linking MBL polymorphisms and TB establishment, paving the way for targeted interventions and a deeper understanding of host-pathogen interactions.
CLEC4E (C-Type Lectin Domain Family 4 Member E)
CLEC4E is a calcium-dependent lectin characterized by carbohydrate recognition domains (CRDs), facilitating its involvement in pathogen recognition and cellular interactions.24 Specifically, CLEC4E encodes the receptor Mincle, situated on the outer membrane of macrophages. Mincle is responsible for recognizing trehalose-6, 6-dimycolate (TDM), a component in the mycobacterial cell wall.25 This recognition triggers signaling cascades within the innate immune system, initiating a robust response to mycobacterial infection.
A single nucleotide polymorphism (SNP) at rs10841847 within CLEC4E has emerged as a crucial determinant in TB susceptibility. The minor allele (G˃A) at this locus is associated with an increased vulnerability to pulmonary TB. This emphasizes the significance of CLEC4E in the context of TB pathogenesis.25 However, the complex landscape of TB susceptibility is likely influenced by multiple genetic factors, necessitating further investigations. While the association between CLEC4E and pulmonary TB is evident, published studies present inconsistent findings. Notably, research in admixed South African populations did not yield statistically significant results, while a study in Northern China reported a decreased predisposition to active TB associated with CLEC4E minor alleles.24,26,27 These discrepancies underscore the need for more comprehensive research to establish the causal link between CLEC4E and TB susceptibility, considering potential confounding factors.
Studies involving mice lacking the Mincle gene offer insights into its role in the immune response against Mycobacterium tuberculosis (Mtb). Depletion of Mincle resulted in the inability to recruit and adhere neutrophils to the site of invasion, impacting the formation of lung granulomas.28 Altered DNA sequences, such as those associated with the rs10841847 SNP, disrupt the normal functioning of Mincle receptors, potentially compromising the ability to bind tubercle glycolipid and increasing susceptibility to TB. Interestingly, studies with knockout mice showed a paradoxical outcome, with a higher bacterial load compared to wild-type mice, suggesting a Mincle-mediated immune response against Mtb.29 This paradox may be attributed to additional genetic factors influencing the sustained immune response, indicating the complexity of host-pathogen interactions in secondary TB.
Pathogen Recognition Receptors (PRRs)
Pathogen recognition receptors are membrane and transmembrane receptors located on the dendritic cells, macrophages, and epithelial cells (exogenous sensors) that recognize different types of Pathogen Associated Molecular Patterns (PAMPs). Macrophage PRRs and phagocytic receptors causative to mycobacterial diseases, especially T.B., have been discussed in several recent reviews.17,24,25 These include cell membrane-bound receptors, such as the mannose receptor (M.R., CD206), dendritic cell-specific ICAM-3-grabbing non-integrin (DC-SIGN) (CD209), Dectin-1, and TLRs. However, in this review, we shall focus on the DC-SIGN and TLRs, which have been associated with Tuberculosis in the African population. This is because they have been adequately studied and have been associated with tuberculosis disease susceptibility and are expressed on many immune cells that recognize numerous molecules of different pathogens including the Mycobacterium tuberculosis.
The exploration of Pathogen Recognition Receptors (PRRs) in dendritic cells, macrophages, and epithelial cells is crucial for deciphering how these receptors recognize diverse Pathogen Associated Molecular Patterns (PAMPs). The emphasis on cell membrane-bound receptors, such as mannose receptor (M.R., CD206), dendritic cell-specific ICAM-3-grabbing non-integrin (DC-SIGN), and Toll-Like Receptors (TLRs), provides a foundation for understanding the initial steps of host-pathogen recognition.30–32
The selective focus on DC-SIGN and TLRs, particularly TLR2, TLR4, and TLR9, is well-justified, considering their extensive associations with TB susceptibility in the African population.31,33,34 These receptors, expressed on various immune cells, serve as critical mediators in the immune response against Mycobacterium tuberculosis. Their well-studied roles in recognizing M. tuberculosis components make them pivotal players in the host defense against TB.35,36
The investigation of Toll-Like Receptors (TLRs) further deepens our understanding of the genetic variants associated with TB susceptibility. The elucidation of TLR1, TLR2, TLR4, and TLR9 variations across different populations provides a nuanced perspective on the global landscape of TB genetics.31 Polymorphisms in these TLRs, including TLR1 G1805T, TLR2 T597C, T1350C, TLR6 C745T, and TLR4 Asp 299Gly, Thr399Ile, reveal potential risk factors for TB susceptibility.31,33,34,37
The signaling pathways initiated by TLR2 and TLR4, leading to the activation of NF-κB and other cascades, are critical in understanding TB susceptibility.35 The identification of specific genetic changes in TLR2, TLR4, and TLR9 associated with TB susceptibility, such as the R753Q variant in TLR2, adds a layer of complexity to our understanding.38 The review delves into the influence of these variants on signaling pathways and their impact on TB progression.
Toll-Like Receptors (TLRs)
Toll-like receptors expressed on various immune cell types, serve as critical mediators in the immune response against a spectrum of pathogens, including Mtb.31,39 Recognizing a diverse array of microbial molecules, TLRs initiate transcription and proinflammatory gene processes. TLRs are categorized based on their cellular localization—surface-bound (eg, TLR2 and TLR4) and intracellular (eg, TLR8 and TLR9).35 The mycobacterial cell wall components are recognized by multiple TLRs, emphasizing their crucial role in the immune response to MTB.34,40
Genetic variants within TLRs have been identified globally, with polymorphisms in TLR1, TLR2, TLR4, TLR8, and TLR9 associated with TB susceptibility.26,31,40 Notably, TLR2 stands out with higher prevalence in genetic variants, forming a heterodimer with TLR1 or TLR6.36 The TLR2 signaling pathway, particularly involving the TIR domain-containing adaptor protein (TIRAP), plays a pivotal role in the inflammatory response to MTB.35,36
In the context of the African population, TLR-2, TLR-4, and TLR-9 emerge as key players in TB susceptibility. The R753Q variant in TLR2 influences disease progression in children.38 Contrasting reports on TLR4 variant D299G highlight its association with TB susceptibility in HIV-infected patients in Tanzania.37,41 The intricate interplay between HIV and TLR variants underscores the multifactorial nature of susceptibility in co-infected individuals. The signaling pathways initiated by TLR2 and TLR4, culminating in the activation of NF-κB, are central to TB susceptibility. Noteworthy changes in these domains correlate with variations in TB susceptibility. The nonsynonymous SNP S180L in TIRAP confers protective signal transduction within TLR2.10 Additionally, TLR7 and TLR8 genetic polymorphisms are associated with TB susceptibility, influencing phagocytosis and immune activation.42 Evidence from TLR9-deficient mice further supports the critical role of TLRs in the innate defense against MTB.26 These results provide proof that TLRs and their signaling moieties in their pathways possess susceptible genes that are associated with Tuberculosis. However, due to variations within individual genes in the different racial populations, it is very hard to make a close linkage of the genetic factors that bring about the association.
DC-SIGN is characterized by a carbohydrate recognition domain (CRD) at its extracellular COOH-terminal end. Its expression on macrophages is influenced by tissue type and activation state.32,39 Notably, DC-SIGN is induced in alveolar macrophages from M. tuberculosis-infected patients, marking its relevance in the context of TB infection.35 The binding of M. tuberculosis to DC-SIGN initiates phagocytosis, allowing the pathogen to enter human monocyte-derived D.C.s. This interaction directly interferes with dendritic cell maturation, contributing to the intricate host-pathogen dynamics.33 The cytoplasmic tail of DC-SIGN, housing three conserved motifs, plays a crucial role in ligand binding, receptor signaling, phagocytosis, and intracellular trafficking of ligand particles.33 This calcium-dependent lectin, known for its affinity for mannose-rich molecules, is expressed predominantly on dendritic cells (D.C.s) and, to varying degrees, on macrophages.34 The dynamic interplay between TB and DC-SIGN involves ligand binding, phagocytosis, and modulation of dendritic cell maturation.32,39
Genetic variations in DC-SIGN have been implicated in TB susceptibility, with polymorphisms in the promoter region (eg, −871A/G and −336A/G) associated with distinct susceptibility patterns (Table 1). Notably, studies in the untranslated regions (UTRs) of CD209 and CD207R genes have revealed variations in gene frequency within African indigenous individuals and the Caucasian American population, underscoring the importance of ethnic, racial, and geographical diversity in TB susceptibility assessment.36 A genetic comparison between African and Eurasian populations has revealed notable disparities, particularly in the frequency of the polymorphic allele −871G. This allele is significantly more prevalent in Eurasians than in Africans, suggesting a genetic migration and close association leading to its introduction into the South African population.43 The absence of haplotypes −871G and −336A in most African populations, except for colored South Africans, further emphasizes the impact of genetic migration on TB susceptibility. In conclusion, such genetic variations tend to influence translation and gene polymorphisms.
Solute Carrier Family 11A, Member 1, SLC11A1 or Natural Resistance-Associated Macrophage Protein 1, or NRAMP1)
The SLC11A1 (NRAMP1) gene encodes a membrane transporter protein whose function is to regulate the cytoplasmic cation levels, especially iron. Iron is essential for the cell to generate reactive oxygen and nitrogen intermediates. It, therefore, acts as a divalent cation transporter across phagosomal membranes.38 The origin of the gene from a mouse is responsible for its resistance to infections by intracellular pathogens, especially the mycobacteria.37
SLC11A1’s function as a divalent cation transporter across phagosomal membranes is critical in modulating the concentration of metal ions within the phagosome. This regulation is paramount for macrophage defense against bacterial infections, specifically by reducing the metal ion concentration where bacterial pathogens reside. A defective NRAMP gene, however, results in increased metal ion accumulation, supporting bacterial growth and compromising the host’s ability to resist infection.
Studies across diverse populations and recent meta-analyses have highlighted the influence of SLC11A1 polymorphisms on TB susceptibility. Four key polymorphisms (3=-UTR, D543N, 5= (G.T.) and INT4 have been extensively studied globally. Although findings exhibit some contradictions in various populations, a meta-analysis in China and an association in Turkey underscore the significance of these polymorphisms in TB development.
A systematic review conducted in China further demonstrates the role of SLC11A1 polymorphisms, particularly at the D543N and INT4 loci, in response to infection rather than solely to Mycobacterium tuberculosis.42,44,45 Additionally, studies in the Gambia suggest potential links between SLC11A1 gene polymorphisms, abnormal iron levels, gene-nutrient interactions, and mortality prediction in HIV-infected patients. This raises intriguing questions about the potential risk of TB development in HIV patients with clinically abnormal iron levels and gene-nutrient interactions. Genetic interactions, such as those observed between TLR2 and polymorphism rs3731865 in African Americans, emphasize the significance of gene-gene interactions in host-pathogen genetic studies. These findings highlight the complexity of allelic heterogeneity within SLC11A1 and underscore the importance of considering various factors in understanding TB susceptibility.
Highlighted associations with SNPs in SLC11A1 are attributed to adjacent SNPs in linkage disequilibrium with reported variants. However, the 5- (G.T.) repeat in the promoter region of SLC11A1 has been shown to affect promoter activity, with allele 3 displaying greater basal and lipopolysaccharides (LPS)-stimulated activity. This intriguing gene activity, although insufficient for establishing clear evidence for in vivo activity, links high activity with resistance and low activity with susceptibility to tuberculosis.46
Chemokines (Chemotactic Cytokines)
Chemokines are a large family of structurally homologous cytokines, secreted proteins that signal through cell surface G protein-coupled heptahelical chemokine receptors that stimulate leukocyte movement and regulate the migration of leukocytes from the blood to tissues. Therefore, chemokines are proinflammatory cytokines of low molecular size, which coordinate the migration and activation of different leukocyte populations. The structurally homologous chemokines are categorized into four groups based on conserved cysteine arrangement: CXC, CC, C, and CX3C. These low molecular-size proinflammatory cytokines play a pivotal role in coordinating the migration and activation of various leukocyte populations.1
Upon activation of alveolar macrophages by intracellular M. tuberculosis, a cascade of chemokines is released. Notable among these are IL-8 (CXCL8), monocyte chemoattractant protein 1 (MCP-1, CCL2), RANTES (CCL5), and CXCL10 (IP-10). These chemokines act as molecular messengers, orchestrating the migration and activation of T cells and macrophages to sites of Mtb infection. This orchestrated response forms the characteristic tuberculous granuloma, a fortress against the dissemination of the organism.2 Systematic reviews and research articles have extensively documented the significance and genetic variations within various chemokines combating Mycobacterium tuberculosis.25,47,48 Polymorphic variations, particularly in the promoter regions of these genes, can modulate transcription and translation, influencing the overall production and activity of chemokines.3,4
The production of chemokines is indispensable for recruiting inflammatory cells to the infection site. Early recruitment of macrophages is pivotal for infection control.5 M. tuberculosis, a potent inducer of chemokines, triggers protective and immunopathogenic host responses. Studies on human macrophages infected in vitro have revealed the induction of CCL2, CCL3, CCL4, and CCL5 in response to virulent mycobacterial strains.49 Regulated upon activation, normal T-cell expressed, and secreted (RANTES) plays a critical role in T-cell activation and macrophage activation.50 Clinical studies have detected the presence of MCP-1, MIP-1a, RANTES, and IP-10 in the serum and bronchoalveolar lavage of TB patients.51 Alveolar macrophages, in particular, produce a distinct profile of chemokines, suggesting a role in the influx of cells to the infection site, and influencing granuloma formation.52 The expression of chemokines by macrophages not only influences TNF-α production but also affects chemokine receptor expression. Specifically, CCL2, CCL3, CCL4, CCL5, CXCL10, and CXCL13 expression is modulated by macrophages in response to Mtb infection.53 Furthermore, TNF-α itself can influence the chemokine network expression, indirectly impacting granuloma formation.54 This intricate interplay extends to mycobacterial cell wall components, regulating the induction of chemokine secretion by macrophages.55
Rantes (Ccl5)
RANTES (regulated upon activation, normal T-cell expressed, and secreted), a member of the C-C chemokine subfamily or beta chemokine. RANTES exhibits chemotactic properties for monocytes, memory T cells, and eosinophils. In addition, it triggers histamine release from human basophils.56,57 Notably, in a murine model, RANTES has been identified as a key player in promoting granuloma formation within M. tuberculosis-infected lungs.56 This process involves the recruitment of immune cells to the infected area, subsequently limiting the intracellular growth of mycobacteria and inducing direct antimicrobial activity, notably through the release of nitric oxide (NO) in alveolar macrophages.58 The protective immunity conferred by RANTES, as evidenced in knockout mice, underscores its significance in the defense against TB.20
Exploring the genetic landscape, the promoter region of the RANTES gene reveals two variants, −403G/A and −28C/G, associated with Tuberculosis (Table 1). These single nucleotide polymorphisms may confer either resistance or susceptibility to TB.59 A recent discovery highlights a functionally important polymorphism, In1.1T/C, located in the intron of RANTES. This polymorphism regulates gene transcription by differentially binding to alternative forms of nuclear proteins. The complexity of RANTES transcription regulation is further unraveled through haplotype analysis. Haplotypes II (A-C-T) and V (G-C-C) exhibit opposing effects on RANTES transcription, with II up-regulating and V down-regulating the process. The luciferase assay, correlating RANTES SNPs with transcription activity, supports this functional insight. Consequently, RANTES concentrations in bronchoalveolar lavage fluid of pulmonary TB patients demonstrate acute elevation during infection and subsequent decline during convalescence. This underscores the dynamic role of RANTES up-regulation in the immune response against M. tuberculosis infection.
Mcp-1 (Ccl2)
The monocyte chemoattractant protein-1, or MCP-1, is a β chemokine and a potent chemotactic factor for monocytes and macrophages. During lung infection by M. tuberculosis, the human monocytes within the body are stimulated to release MCP-1.60 During the host M. tuberculosis-specific immune response, MCP-1 participates in the inhibition of the in vivo dissemination of M. Tuberculosis regulating the secondary immune response. Therefore, MCP-1 is a vital promoter and regulator of a host’s defense against Tuberculosis infection. However, experimental studies in mice have shown that a deficiency in the chemokine MCP-1 alters the monocyte recruitment and formation of the granuloma, and yet it has the advantage of decreased M. Tuberculosis susceptibility.41 Studies on genotype and allele frequencies especially at the locus −2518 have shown contradictory results and have not yielded concrete and adequate proof for the effects of the polymorphisms in the MCP-1 gene. However, the carriers of the −2518 GG genotype were reported to produce high levels of MCP-1, which inhibits IL-12 production in response to M. Tuberculosis and promotes active pulmonary T.B.,61 whereas Thye et al62 initially found the association with the −2518G allele with T.B. resistance in Ghana, and further genotyping analysis using Microarray technology identified −362C allele as the only true protective variant of MCP-1, with a linkage disequilibrium in the region of −2518 and-362. This study is a deterrent note for the need to carry out a comprehensive genetic investigation to search for the actual cause of the polymorphism that exists in the variant and gene of interest.
Conclusion
In summary, the exploration of genetic factors influencing tuberculosis susceptibility in African populations represents a significant step forward in our understanding of the complex interplay between host genetics and infectious diseases. The comprehensive analysis presented in this article delves into the polymorphisms within immune genes and their association with TB susceptibility specifically within the African context. This study contributes valuable insights into the genetic landscape of TB susceptibility in African populations. By focusing on this region, the research sheds light on population-specific genetic variants that may play a pivotal role in determining an individual’s susceptibility to TB.
One key research gap pertains to the lack of comprehensive studies that consider the diverse genetic, environmental, and socio-economic factors influencing TB outcomes across different African populations. Existing research often fails to adequately account for the genetic diversity present within African populations, leading to inconsistent findings and limited generalizability of results. Moreover, there is a scarcity of longitudinal studies that can elucidate the temporal dynamics of TB susceptibility and progression in African populations, hindering our understanding of the disease’s trajectory and the efficacy of interventions over time.
Additionally, the reliance on small sample sizes and single-center studies limits the statistical power and reliability of findings, further exacerbating the inconsistency of outcomes observed in earlier research efforts. Furthermore, there is a scarcity of studies that integrate genetic, environmental, and socio-economic data to comprehensively assess the determinants of TB susceptibility in African populations, impeding our ability to develop targeted interventions tailored to the specific needs of these populations.
To address these research gaps and enhance our understanding of TB susceptibility in African populations, we propose several suggestions for further similar research. Firstly, there is a need for larger, multicenter studies that encompass diverse African populations to ensure the generalizability of findings and account for population-specific factors. Such studies should employ longitudinal designs to capture the temporal dynamics of TB susceptibility and progression, allowing for the identification of predictive biomarkers and the evaluation of interventions over time.
Moreover, future research efforts should prioritize the integration of genetic, environmental, and socio-economic data through interdisciplinary collaborations between geneticists, epidemiologists, clinicians, and social scientists. This holistic approach will provide a more nuanced understanding of the complex interactions underlying TB susceptibility in African populations and inform the development of targeted interventions that address the multifactorial nature of the disease.
Furthermore, leveraging emerging technologies such as genomic sequencing, big data analytics, and machine learning algorithms can facilitate the identification of novel genetic determinants and biomarkers associated with TB susceptibility in African populations. By harnessing these innovative approaches, researchers can overcome the limitations of earlier studies and advance our understanding of TB epidemiology in Africa, ultimately contributing to the development of effective strategies for TB prevention, diagnosis, and treatment tailored to the specific needs of African populations.
Abbreviations
MHC, Major histocompatibility complex; SLC11A1, Solute carrier family 11a member 1; HLA, Human leukocyte antigen; VDR, Vitamin D nuclear receptor; TNF, Tumour necrosis factor; IRGM, Immunity-related GTPase family M protein; SNP, Single Nucleotide Polymorphism; MTBC, Mycobacterium tuberculosis complex; MCP-1, Monocyte chemoattractant protein 1; MBL2, Mannose-binding lectin 2 gene; Mtb, Mycobacterium tuberculosis; NRAMP1, Natural resistance Associated Macrophage Protein 1 gene; SP-A, Surfactant protein A; SP-D, Surfactant protein D; CRD, Carbohydrate recognition domain; RANTES, Regulated upon activation, normal T-cell expressed, and secreted; TB, Tuberculosis; TLR, Toll-like receptor; DC-SIGN, Dendritic Cell-Specific Intercellular adhesion molecule-3 grabbing non-integrin; WHO, World Health Organization; PRR, Pathogen Recognition Receptor; PAMP, Pathogen Associated Molecular Pattern; CLEC4E, C-type Lectin Domain Family 4 Member E; IL, Interleukin; NO, Nitric Oxide.
Data Sharing Statement
All data generated by this manuscript has been integrated into the manuscript.
Acknowledgments
We are thankful to the Makerere University Library for the provision of electronic information resources that enabled us to complete the review article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that this research project was funded by the Africa Centre of Excellence in Materials, Product Development & Nanotechnology; MAPRONANO ACE, Grant No. P151847IDA credit 5797-UG, College of Engineering Design Art and Technology, Makerere University.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Harding E. WHO global progress report on tuberculosis elimination. Lancet Respir Med. 2020;8(1):19. doi:10.1016/S2213-2600(19)30418-7
2. Dye C, Reeder JC, Terry RF. Research for universal health coverage. Sci Transl Med. 2013;5(199):199ed13. doi:10.1126/scitranslmed.3006971
3. Barreiro LB, Neyrolles O, Babb CL, et al. Promoter variation in the DC-SIGN-encoding gene CD209 is associated with tuberculosis. PLoS Med. 2006;3(2):e20. doi:10.1371/journal.pmed.0030020
4. Ben-Ali M, Barreiro LB, Chabbou A, et al. Promoter and neck region length variation of DC-SIGN is not associated with susceptibility to tuberculosis in Tunisian patients. Hum Immunol. 2007;68(11):908–912. doi:10.1016/j.humimm.2007.09.003
5. Yim JJ, Selvaraj P. Genetic susceptibility in tuberculosis. Respirology. 2010;15(2):241–256. doi:10.1111/j.1440-1843.2009.01690.x
6. Pepperell CS, Casto AM, Kitchen A, et al. The role of selection in shaping diversity of natural M. tuberculosis populations. PLoS Pathog. 2013;9(8):e1003543. doi:10.1371/journal.ppat.1003543
7. World Health Organization, Global Tuberculosis Report; 2020.
8. Campbell MC, Tishkoff SA. African genetic diversity: implications for human demographic history, modern human origins, and complex disease mapping. Annu Rev Genomics Hum Genet. 2008;9(1):403–433. doi:10.1146/annurev.genom.9.081307.164258
9. Gray JM, Cohn DL. Tuberculosis and HIV coinfection. Semin Respir Crit Care Med. 2013;34(1):32–43. doi:10.1055/s-0032-1333469
10. Harling G, Ehrlich R, Myer L. The social epidemiology of tuberculosis in South Africa: a multilevel analysis. Soc Sci Med. 2008;66(2):492–505. doi:10.1016/j.socscimed.2007.08.026
11. Oga-Omenka C, Tseja-Akinrin A, Sen P, et al. Factors influencing diagnosis and treatment initiation for multidrug-resistant/rifampicin-resistant tuberculosis in six sub-Saharan African countries: a mixed-methods systematic review. BMJ Glob Health. 2020;5(7):e002280. doi:10.1136/bmjgh-2019-002280
12. Andrews JR, Shah N, Gandhi N, et al. Multidrug-resistant and extensively drug-resistant tuberculosis: implications for the HIV epidemic and antiretroviral therapy rollout in South Africa. J Infect Dis. 2007;196(Suppl s3):S482–90. doi:10.1086/521121
14. Chakaya J, Khan M, Ntoumi F, et al. Global Tuberculosis Report 2020 – Reflections on the Global TB burden, treatment and prevention efforts. Int J Infect Dis. 2021;113(Suppl 1):S7–s12. doi:10.1016/j.ijid.2021.02.107
15. Selvaraj P, Uma H, Reetha AM, et al. HLA antigen profile in pulmonary tuberculosis patients & their spouses. Indian J Med Res. 1998;107:155–158.
16. Singh SP, Mehra NK, Dingley HB, et al. Human leukocyte antigen (HLA)-linked control of susceptibility to pulmonary tuberculosis and association with HLA-DR types. J Infect Dis. 1983;148(4):676–681. doi:10.1093/infdis/148.4.676
17. Torrelles JB, Torrelles J, Azad A, et al. Role of C-type lectins in mycobacterial infections. Curr Drug Targets. 2008;9(2):102–112. doi:10.2174/138945008783502467
18. Beharka AA, Gaynor CD, Kang BK, et al. Pulmonary surfactant protein A up-regulates activity of the mannose receptor, a pattern recognition receptor expressed on human macrophages. J Immunol. 2002;169(7):3565–3573. doi:10.4049/jimmunol.169.7.3565
19. Ferguson JS, Voelker DR, McCormack FX, et al. Surfactant Protein D Binds to Mycobacterium tuberculosis Bacilli and Lipoarabinomannan via Carbohydrate-Lectin Interactions Resulting in Reduced Phagocytosis of the Bacteria by Macrophages1. J Immunol. 1999;163(1):312–321. doi:10.4049/jimmunol.163.1.312
20. Salam N, Gupta S, Sharma S, et al. Protective immunity to Mycobacterium tuberculosis infection by chemokine and cytokine conditioned CFP-10 differentiated dendritic cells. PLoS One. 2008;3(8):e2869. doi:10.1371/journal.pone.0002869
21. Vieira F, Kung JW, Bhatti F. Structure, genetics and function of the pulmonary associated surfactant proteins A and D: the extra-pulmonary role of these C type lectins. Ann Anat. 2017;211:184–201. doi:10.1016/j.aanat.2017.03.002
22. Naqvi KF, Endsley JJ. Myeloid C-type lectin receptors in tuberculosis and HIV immunity: insights into co-infection? Front Cell Infect Microbiol. 2020;10:263. doi:10.3389/fcimb.2020.00263
23. Garred P, Larsen F, Seyfarth J, et al. Mannose-binding lectin and its genetic variants. Genes Immun. 2006;7(2):85–94. doi:10.1038/sj.gene.6364283
24. Jo EK. Mycobacterial interaction with innate receptors: tLRs, C-type lectins, and NLRs. Curr Opin Infect Dis. 2008;21(3):279–286. doi:10.1097/QCO.0b013e3282f88b5d
25. Sasindran SJ, Torrelles JB. Mycobacterium Tuberculosis Infection and Inflammation: what is Beneficial for the Host and for the Bacterium? Front Microbiol. 2011;2:2. doi:10.3389/fmicb.2011.00002
26. Carvalho NB, Oliveira FS, Duraes FV, et al. Toll-like receptor 9 is required for full host resistance to mycobacterium avium infection but plays no role in induction of Th1 Responses. Infect Immun. 2011;79(4):1638–1646. doi:10.1128/IAI.01030-10
27. Bowker N, Salie M, Schurz H, et al. Polymorphisms in the pattern recognition receptor mincle gene (CLEC4E) and association with tuberculosis. Lung. 2016;194(5):763–767. doi:10.1007/s00408-016-9915-y
28. Lai YF, Lin T-M, Wang C-H, et al. Functional polymorphisms of the TLR7 and TLR8 genes contribute to Mycobacterium tuberculosis infection. Tuberculosis. 2016;98:125–131. doi:10.1016/j.tube.2016.03.008
29. Mortaz E, Adcock IM, Tabarsi P, et al. Interaction of Pattern Recognition Receptors with Mycobacterium Tuberculosis. J Clin Immunol. 2015;35(1):1–10. doi:10.1007/s10875-014-0103-7
30. Olvany JM, Sausville LN, White MJ, et al. CLEC4E (Mincle) genetic variation associates with pulmonary tuberculosis in Guinea-Bissau (West Africa). Infect Genet Evol. 2020;85:104560. doi:10.1016/j.meegid.2020.104560
31. Zhang Y, Jiang T, Yang X, et al. Toll-like receptor −1, −2, and −6 polymorphisms and pulmonary tuberculosis susceptibility: a systematic review and meta-analysis. PLoS One. 2013;8(5):e63357. doi:10.1371/journal.pone.0063357
32. Puig-Kröger A, Serrano-Gómez D, Caparrós E, et al. Regulated expression of the pathogen receptor dendritic cell-specific intercellular adhesion molecule 3 (ICAM-3)-grabbing nonintegrin in THP-1 human leukemic cells, monocytes, and macrophages. J Biol Chem. 2004;279(24):25680–25688. doi:10.1074/jbc.M311516200
33. Azad AK, Torrelles JB, Schlesinger LS. Mutation in the DC-SIGN cytoplasmic triacidic cluster motif markedly attenuates receptor activity for phagocytosis and endocytosis of mannose-containing ligands by human myeloid cells. J Leukoc Biol. 2008;84(6):1594–1603. doi:10.1189/jlb.0308192
34. Barreiro LB, Ben-Ali M, Quach H, et al. Evolutionary dynamics of human Toll-like receptors and their different contributions to host defense. PLoS Genet. 2009;5(7):e1000562. doi:10.1371/journal.pgen.1000562
35. Tailleux L, Pham-Thi N, Bergeron-Lafaurie A, et al. DC-SIGN induction in alveolar macrophages defines privileged target host cells for mycobacteria in patients with tuberculosis. PLoS Med. 2005;2(12):e381. doi:10.1371/journal.pmed.0020381
36. Boily-Larouche G, Zijenah LS, Mbizvo M, et al. DC-SIGN and DC-SIGNR genetic diversity among different ethnic populations: potential implications for pathogen recognition and disease susceptibility. Hum Immunol. 2007;68(6):523–530. doi:10.1016/j.humimm.2007.02.002
37. Vidal SM, Malo D, Vogan K, et al. Natural resistance to infection with intracellular parasites: isolation of a candidate for Bcg. Cell. 1993;73(3):469–485. doi:10.1016/0092-8674(93)90135-D
38. Gruenheid S, Pinner E, Desjardins M, et al. Natural resistance to infection with intracellular pathogens: the nramp1 protein is recruited to the membrane of the phagosome. J Exp Med. 1997;185(4):717–730. doi:10.1084/jem.185.4.717
39. Serrano-Gómez D, Dominguez-Soto A, Ancochea J, et al. Dendritic cell-specific intercellular adhesion molecule 3-grabbing nonintegrin mediates binding and internalization of aspergillus fumigatus conidia by dendritic cells and macrophages. J Immunol. 2004;173(9):5635–5643. doi:10.4049/jimmunol.173.9.5635
40. Quesniaux VJ, Nicolle DM, Torres D, et al. Toll-like receptor 2 (TLR2)-dependent-positive and TLR2-independent-negative regulation of proinflammatory cytokines by mycobacterial lipomannans. J Immunol. 2004;172(7):4425–4434. doi:10.4049/jimmunol.172.7.4425
41. Lu B, Rutledge BJ, Gu L, et al. Abnormalities in monocyte recruitment and cytokine expression in monocyte chemoattractant protein 1-deficient mice. J Exp Med. 1998;187(4):601–608. doi:10.1084/jem.187.4.601
42. Li HT, Zhang TT, Zhou YQ, et al. SLC11A1 (formerly NRAMP1) gene polymorphisms and tuberculosis susceptibility: a meta-analysis. Int J Tuberc Lung Dis. 2006;10(1):3–12.
43. Blackwell JM, Jamieson SE, Burgner D. HLA and infectious diseases. Clin Microbiol Rev. 2009;22(2):370–385. doi:10.1128/CMR.00048-08
44. Ates O, Dalyan L, Müsellim B, et al. NRAMP1 (SLC11A1) gene polymorphisms that correlate with autoimmune versus infectious disease susceptibility in tuberculosis and rheumatoid arthritis. Int J Immunogenet. 2009;36(1):15–19. doi:10.1111/j.1744-313X.2008.00814.x
45. Song W, Li D, Tao L, et al. Solute carrier transporters: the metabolic gatekeepers of immune cells. Acta Pharm Sin B. 2020;10(1):61–78. doi:10.1016/j.apsb.2019.12.006
46. Searle S, Blackwell JM. Evidence for a functional repeat polymorphism in the promoter of the human NRAMP1 gene that correlates with autoimmune versus infectious disease susceptibility. J Med Genet. 1999;36(4):295–299. doi:10.1136/jmg.36.4.295
47. Berrington WR, Hawn TR. Mycobacterium tuberculosis, macrophages, and the innate immune response: does common variation matter? Immunol Rev. 2007;219(1):167–186. doi:10.1111/j.1600-065X.2007.00545.x
48. Selvaraj P, Alagarasu K, Harishankar M, et al. Cytokine gene polymorphisms and cytokine levels in pulmonary tuberculosis. Cytokine. 2008;43(1):26–33. doi:10.1016/j.cyto.2008.04.011
49. Ben-Ali M, Barbouche M-R, Bousnina S, et al. Toll-like receptor 2 Arg677Trp polymorphism is associated with susceptibility to tuberculosis in Tunisian patients. Clin Diagn Lab Immunol. 2004;11(3):625–626. doi:10.1128/CDLI.11.3.625-626.2004
50. Velez DR, Wejse C, Stryjewski ME, et al. Variants in toll-like receptors 2 and 9 influence susceptibility to pulmonary tuberculosis in Caucasians, African-Americans, and West Africans. Hum Genet. 2010;127(1):65–73. doi:10.1007/s00439-009-0741-7
51. Newport MJ, Allen A, Awomoyi AA, et al. The toll-like receptor 4 Asp299Gly variant: no influence on LPS responsiveness or susceptibility to pulmonary tuberculosis in The Gambia. Tuberculosis. 2004;84(6):347–352. doi:10.1016/j.tube.2004.02.001
52. Olesen R, Wejse C, Velez DR, et al. DC-SIGN (CD209), pentraxin 3 and vitamin D receptor gene variants associate with pulmonary tuberculosis risk in West Africans. Genes Immun. 2007;8(6):456–467. doi:10.1038/sj.gene.6364410
53. Khor CC, Chapman SJ, Vannberg FO, et al. A Mal functional variant is associated with protection against invasive pneumococcal disease, bacteremia, malaria and tuberculosis. Nat Genet. 2007;39(4):523–528. doi:10.1038/ng1976
54. Jones BW. Differential roles of Toll-like receptors in the elicitation of proinflammatory responses by macrophages. Ann Rheum Dis. 2001;60(Suppl 3):6–12. doi:10.1136/ard.60.1.6
55. Fitness J, Hill A, Fine P, et al. Large-scale candidate gene study of leprosy susceptibility in the Karonga district of northern Malawi. Am J Trop Med Hyg. 2004;71(3):330–340. doi:10.4269/ajtmh.2004.71.330
56. Chensue SW, Warmington KS, Allenspach EJ, et al. Differential expression and cross-regulatory function of RANTES during mycobacterial (type 1) and schistosomal (type 2) antigen-elicited granulomatous inflammation. J Immunol. 1999;163(1):165–173. doi:10.4049/jimmunol.163.1.165
57. van Crevel R, Ottenhoff TH, Van Der Meer JW. Innate immunity to Mycobacterium tuberculosis. Clin Microbiol Rev. 2002;15(2):294–309. doi:10.1128/CMR.15.2.294-309.2002
58. Saukkonen JJ, Bazydlo B, Thomas M, et al. β-Chemokines Are Induced by Mycobacterium tuberculosis and Inhibit Its Growth. Infect Immun. 2002;70(4):1684–1693. doi:10.1128/IAI.70.4.1684-1693.2002
59. Ben-Selma W, Harizi H, Bougmiza I, et al. Polymorphisms in the RANTES Gene Increase Susceptibility to Active Tuberculosis in Tunisia. DNA Cell Biol. 2011;30(10):789–800. doi:10.1089/dna.2010.1200
60. Lin Y, Gong J, Zhang M, et al. Production of monocyte chemoattractant protein 1 in tuberculosis patients. Infect Immun. 1998;66(5):2319–2322. doi:10.1128/IAI.66.5.2319-2322.1998
61. Flores-Villanueva PO, Ruiz-Morales JA, Song C-H, et al. A functional promoter polymorphism in monocyte chemoattractant protein–1 is associated with increased susceptibility to pulmonary tuberculosis. J Exp Med. 2005;202(12):1649–1658. doi:10.1084/jem.20050126
62. Thye T, Nejentsev S, Intemann CD, et al. MCP-1 promoter variant −362C associated with protection from pulmonary tuberculosis in Ghana, West Africa. Hum Mol Genet. 2009;18(2):381–388. doi:10.1093/hmg/ddn352
Hypertension is the most common risk factor for cardiovascular diseases (CVDs).1 Globally it affects about 40% of the population and causes approximately 7.6 million deaths every year.2 Despite the availability of effective interventions, including antihypertensive medication only 20% with hypertension have well-controlled blood pressure.3 In Nepal, high blood pressure was the leading cause of CVDs in 20174 where 20–30% of adult women and men have hypertension.5 The high proportion of untreated (89% of those aware) and uncontrolled (96% of those on treatment) hypertension in Nepal,5 jeopardizes the government’s commitment to reduce CVDs.6
Management of hypertension may require substantial efforts, including adherence to antihypertensive medications, monitoring of blood pressure, frequent follow-up with healthcare providers, weight reduction, physical activity, healthy diet, and avoidance of alcohol and tobacco use.7 Patients with chronic conditions like hypertension often need social and family support to optimally manage their ailment.8,9 Social support is a multidimensional concept often defined as activities and relationships that individuals receive and provide to each other within their social networks.10 A large and diverse social support network can boost self-esteem and provide better access to information and resources.11,12 Health-related interactions with friends and family promote healthy behaviors including adherence to treatment.13–16 Feeling connected with others and the awareness that support is available when needed are important for positive health outcomes.17–19 Positive social relationships help patients cope with illness associated stress promoting better prognosis.20 Social support may protect patients from complications by helping with health management,16 or by encouraging healthy behaviors.21 However, the evidence on the role of social support in the management of chronic conditions is inconclusive. Studies have shown a positive,22–26 null27,28 and an inverse association29 between social support and management of chronic conditions. The role of social support in the management of chronic conditions like hypertension has not been sufficiently explored in the Nepalese context. One study from Nepal reported a positive association between social support and self-care for hypertension.30 In this study, we explored how perceived social support influences medication adherence and control of high blood pressure. The results from this study could serve to inform targeted community-based interventions according to the level of social support received by hypertension patients for controlling hypertension.
Materials and Methods
Study Setting
The study was conducted in Budhanilkantha municipality, Kathmandu, Nepal. The municipality has nearly 150,000 inhabitants31 and has 11 public health facilities that provide primary health care and tertiary care is provided by the private and public hospitals nearby. Hypertension prevalence of the urban areas such as Budanilakantha (25.2%) is similar to the national average (24.5%).5
Study Design and Population
Cross-sectional data collected at baseline from 1252 hypertensive individuals enrolled in a cluster randomized trial (Registration no: NCT05292469). The detailed trial methods are published elsewhere.32 Trained enumerators identified participants seeking support from health workers and volunteers, screened for eligibility, and obtained written informed consent after explaining the trial objectives. Eighteen years and older individuals with established hypertension diagnosis (systolic BP ≥140 mmHg and/or diastolic BP ≥ 90 mmHg on at least two consecutive visits or using antihypertensive medication) and able to respond to the questions were recruited. Pregnant women were excluded.
Data Collection
Trained enumerators collected baseline data from 2 May 2022 through 7 November 2022 using an android operating system tablet installed with KOBO toolbox electronic data collection platform. The questionnaire was pretested. Participants were shown picture cards with examples of physical activity and commonly used utensils for drinking alcohol to ensure accurate measurements.5
Outcomes
Hypertension control
An “Omron” digital instrument was used to measure blood pressure three times in a resting position and the mean of the last two measurements was registered. Participants with systolic and diastolic blood pressure less than 140 and 90 mmHg were categorized as controlled hypertension others as uncontrolled hypertension.
Medication adherence
We administered an eight-item Morisky Medication Adherence Scale (MMAS-8) (Supplementary Table 1).33 The scale is widely used to measure medication adherence and is reported to have good reliability (α = 0.83) and validity with sensitivity of 93% and specificity of 53% for low adherence.34 The first seven questions have responses YES coded as 0 and NO coded as 1. The code of the fifth question was reversed and the responses to the eighth question were re-coded from 2 to 0.75, 3 to 0.5, 4 to 0.25, 5 to 0 during the analysis. Responses to all eight questions were added to get MMAS, and a score above 6 was considered good adherence and ≤6 poor adherence.35
Exposures
Modified multidimensional scale of perceived social support (MSPSS) was used to measure the adequacy of support participants received from family, friends, and significant others (Supplementary Table 2).36 Twelve questions with answers on a 5-point Likert scale (1 = strongly disagree; 5=strongly agree) were asked to the participants. Cronbach’s alpha has been estimated to be 0.92, 0.85, 0.85 and 0.86 for total and family, friends, and significant others subscales, respectively.36 The MSPSS was translated into Nepali by SB and was reviewed by the study clinician. During training, the wording of the questions was discussed with the enumerators from the study community. The enumerators pretested the questions, and any problems encountered in administering the questions were discussed and addressed before finalizing the tool. The internal consistency reliability for the MSPSS was found good with a Cronbach’s alpha of 0.91 for the overall score and 0.87, 0.91, and 0.84 for family, friend, and significant other subscales, respectively. The overall MSPSS ranged between 12 and 60, high scores indicate high perceived social support. The subscale scores were calculated by adding the responses for related questions. During analysis, scores were divided by the number of questions included in each scale resulting in scores ranging between 1 and 5. The scores were categorized as low (1.00–3.59), moderate (3.60–4.59), and high (4.60–5.00) support.
Covariates
The covariates included in the model were age (continuous), gender (female/male), ethnicity (Brahmin Chettri/Newars/Tamang, Sherpa, Rai, Gurung, Magar/Dalits), current marital status (unmarried/married), education (illiterate/primary/secondary/high school and above), and per capita annual income in US dollars (continuous). Other variables considered were occupation status (unemployed/paid employment), self-reported diabetes status (status not known/non-diabetic/diabetic), years since hypertension diagnosis, and prescribed antihypertensives (Yes/No). The diet quality questionnaire assessed 32 different food groups participants ate in the 24 hours preceding the survey.37 The global dietary recommendation score (ranging from 0 to 18, higher score means better diet quality) was calculated by subtracting foods recommended to limit from foods recommended as healthy and adding nine. It measures adherence to a healthy diet protective against non-communicable diseases.37 Fruits and vegetable scores ranged from 0 to 6, with scores of <3 indicate the likelihood of eating less than 400 grams of fruits and vegetables.37 Daily salt intake was asked and categorized as ≤10 grams, 11–15 grams, and >15 grams. A global physical activity questionnaire38 was used to calculate metabolic equivalents of task (METs) minutes per week categorizing <600 METs (inadequate) and ≥600 (adequate). Body mass index of <25 kg/m2 and ≥25 kg/m2 was categorized as normal weight and overweight, respectively.39 Standard drinks per week were calculated by asking current alcohol drinkers about drinking frequency and amount of different types of alcohol5 and categorizing into non-drinkers (≤1 standard drink per month), moderate drinkers (<3 standard drinks per week), and high drinkers (≥3 standard drinks per week). Tobacco use including both smoked and chewed was categorized as never, and ever users.
Statistical Analysis
Descriptive statistics were presented as frequencies and percentages for categorical variables and mean and standard deviation for continuous variables. Confounders included in the model were identified a priori by constructing a directed acyclic graph (DAG)40 to assess the association between MSPSS and controlled hypertension and adherence to antihypertensives. We fitted Poisson regression to assess the association between MSPSS and hypertension control. Prevalence ratios and corresponding 95% confidence intervals were estimated. Two models were fitted, unadjusted (model 1) and adjusted for age, gender, ethnicity, marital status, education, and income (model 2). Similar models were also fitted to assess the association between MSPSS and adherence to antihypertensives. Based on the DAGs, mediators such as dietary, lifestyle and clinical factors were not included in the model. All analyses were performed with Stata 18.41
Ethics
We have obtained ethical approval from Nepal Health Research Council (Protocol number: 682/2021) approved on 24 December 2021 and Regional Committee for Medical and Health Research Ethics, Norway (Reference number: 399479) approved on 22 February 2022. We have adhered to the declaration of Helsinki throughout the research process.
Results
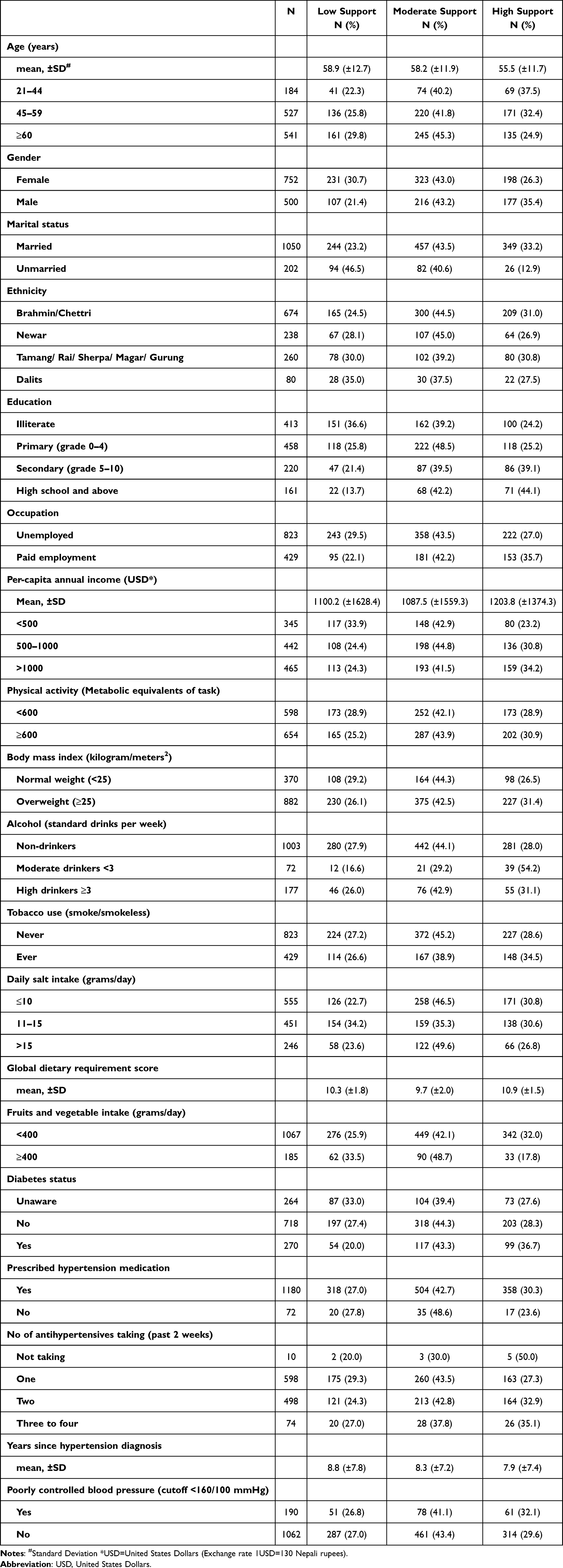
The mean age of study participants was 57.5 years, and 60% were females. Table 1 shows the distribution of sociodemographic, lifestyle and clinical factors by categories of overall MSPSS. Participants with high social support were generally younger and more often males, married, belonged to Brahmin/Chettri ethnicity, were highly educated, had paid employment, had high per capita income, physically active, overweight, drink <3 standard drinks per week, current tobacco users, consumed daily <10 grams salt, had high global dietary requirement score, consumed less fruits and vegetables, were diabetic, were prescribed more than three antihypertensives, had shorter duration since diagnosis of hypertension and had poorly controlled blood pressure.
Table 1 Socioeconomic, Lifestyle, and Clinical Factors by Levels of Overall MSPSS
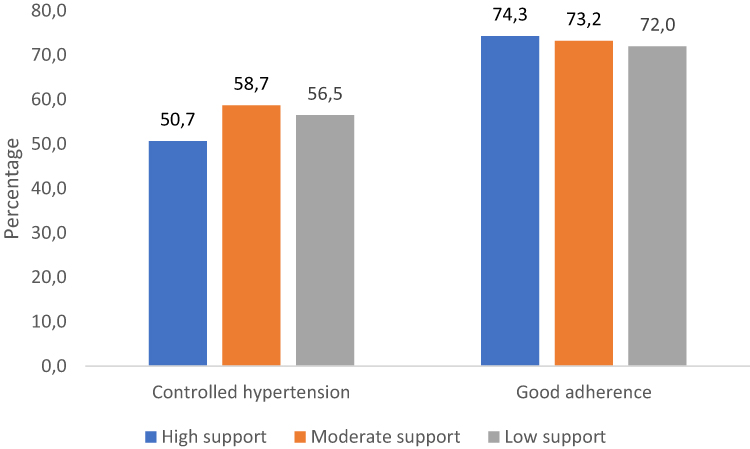
Out of the 1252 participants 914 (73%) reported receiving moderate to high overall MSPSS. Figure 1 shows that the high proportion of individuals with controlled hypertension and good adherence to antihypertensives were in moderate MSPSS category (58.7%) and high MSPSS category (74.3%), respectively. The distribution of MSPSS subscales by status of hypertension control and adherence to antihypertensives are shown in Supplementary Tables 3 and 4.
Figure 1 Proportion controlling hypertension and good adherence to antihypertensives in categories of overall MSPSS.
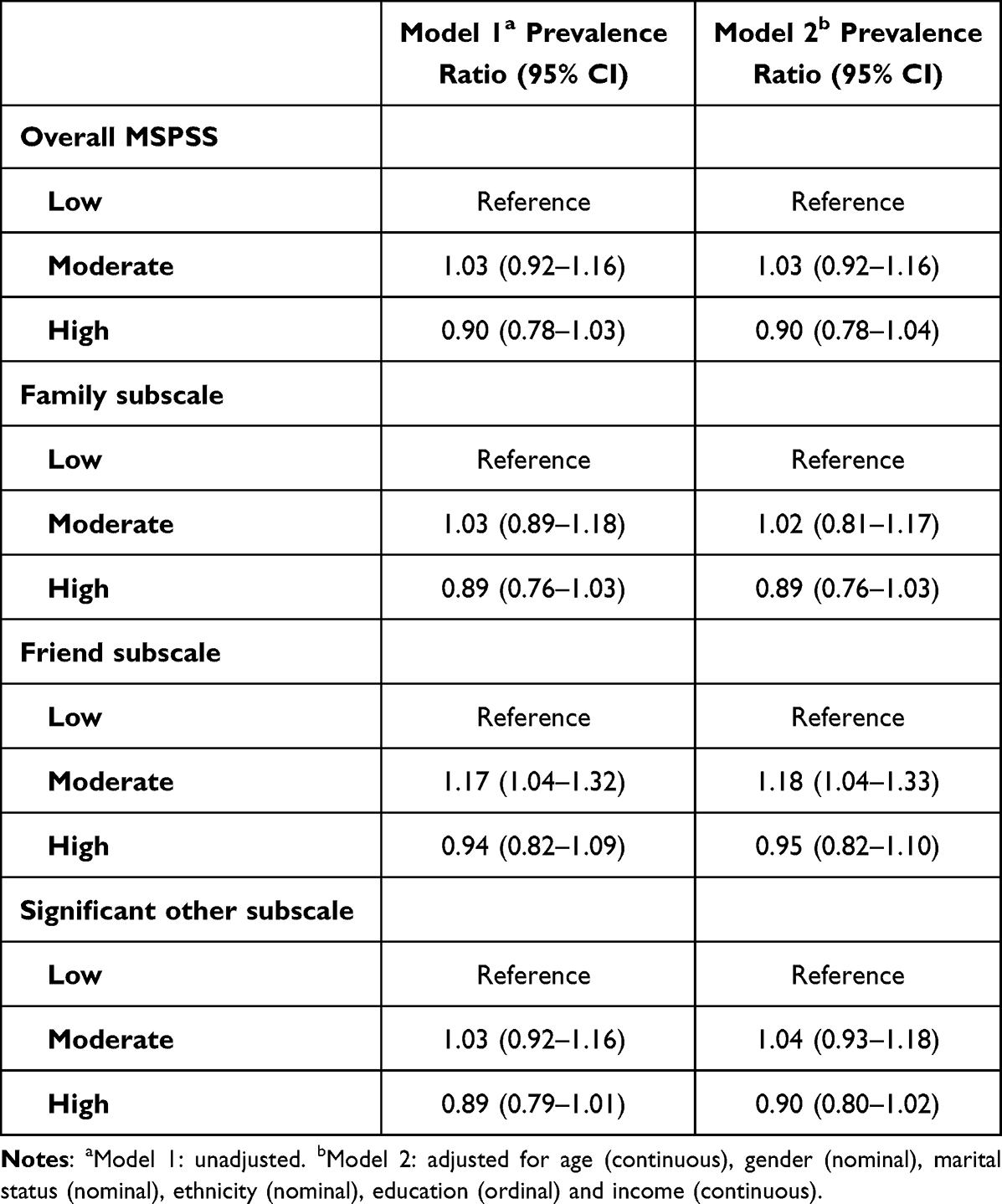
Overall, there was no significant association between social support and controlled hypertension (Table 2). However, individuals who received a moderate level of social support from friends exhibited 1.18 (95% CI, 1.04–1.33) times higher prevalence of controlled hypertension compared to those receiving low support.
Table 2 Association Between MSPSS and Controlled Hypertension
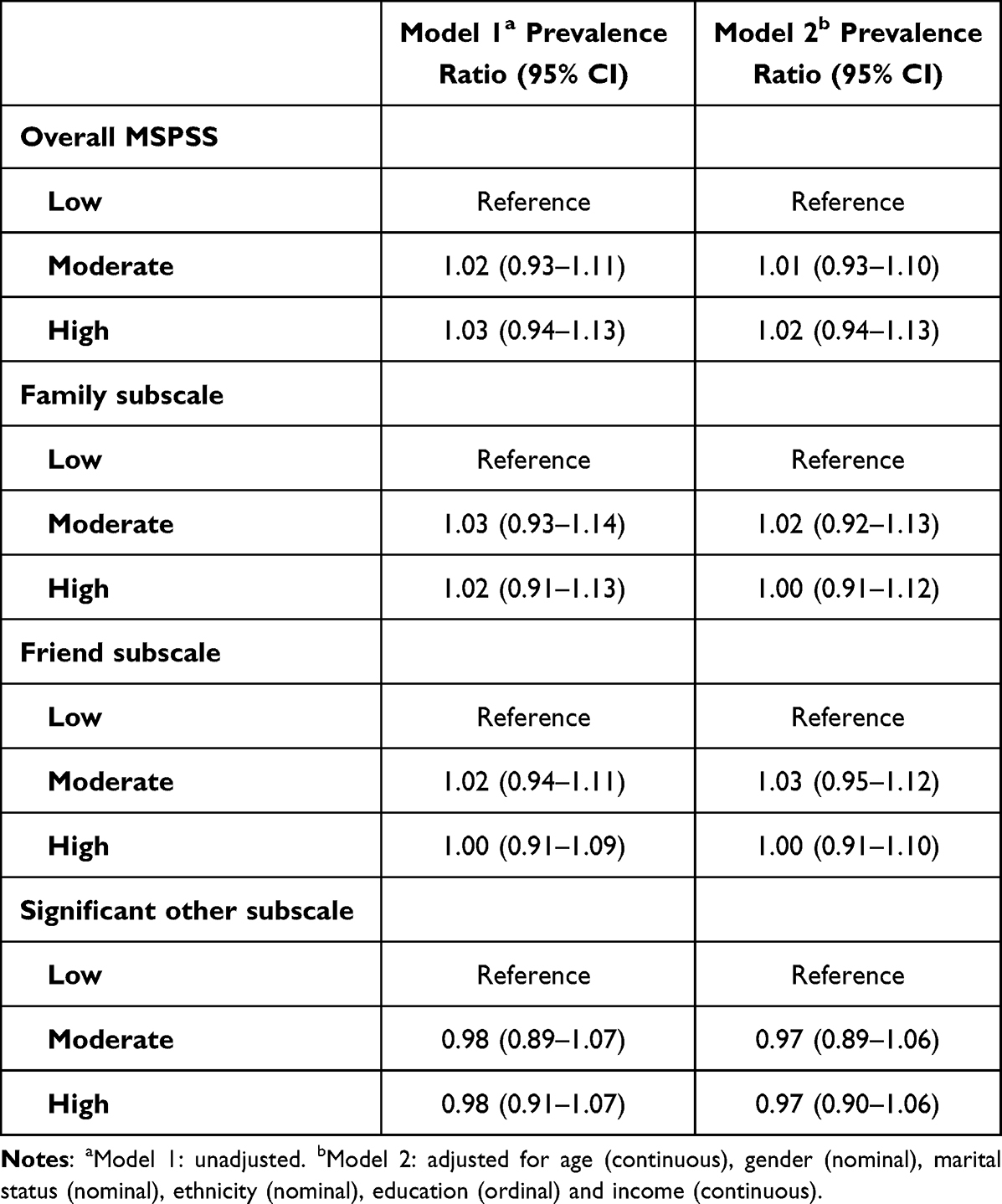
Further, Table 3 shows that there was no association between social support and prevalence of adherence to antihypertensives, and unadjusted and adjusted estimates were very similar.
Table 3 Association Between MSPSS and Adherence to Antihypertensives
Discussion
In this study, we explored how perceived social support received by hypertension patients affected adherence to antihypertensives and control of hypertension. Our analysis showed that 73% of participants received moderate to high social support. Despite anticipating a positive association between MSPSS and controlled hypertension, we found that participants in the high MSPSS category had the lowest proportion of hypertension control (51%) while the proportion of good adherence did not differ between MSPSS categories. There was no association between MSPSS and adherence to antihypertensives and controlled hypertension except for friend’s sub-scale where higher prevalence of controlled hypertension was observed in moderate social support compared to low.
Very few studies from Nepal have reported on the relationship between social support and hypertension control and adherence to antihypertensives. Our finding that hypertensive patients receive high social support is in line with previous studies from Ethiopia42 and Turkey,43 but not with studies from Nepal30 and Malaysia.44 Previous studies from high-income countries agree with our findings that social support is neither associated with hypertension control45,46 (Spain/Korea) nor with adherence to antihypertensives28 (USA). However, a positive association between social support with controlled hypertension has been reported by a study from Vietnam47 and with adherence to antihypertensives by studies from India,23 China48 and Turkey.43 The inconsistent findings could be due to discrepancies in how social support was measured. A few studies have used MSPSS30,43,49 to measure social support but their outcome measure was self-efficacy to hypertension rather than hypertension control while those with hypertension control as the outcome measured social support differently by measuring frequency of visits by friends and family,45 social support inventory,28 self-esteem and belongingness23 and availability of informational, emotional, practical support.27,46,48
The quality and type of social support received has a bearing on adherence to medication and hypertension control.13 Practical support received for household chores lowered the risk of uncontrolled hypertension in Vietnam,47 whereas financial support from friends was harmful to adherence to medication in China.48 Therefore, nuanced studies disentangling the mechanisms through which social support the process of hypertension management are needed.
The reason hypertensive patients received high social support in our study may be due to availability of family members rendered by large family size in our sample. Despite the high level of support received by participants, we did not observe a significant positive association between MSPSS and hypertension control and adherence to antihypertensives. This may be due to a tendency of parents not wanting to burden children with their health concerns.50 Also, nearly 33% of the participants were illiterate and their friends and family are likely similar. Even when support is available, a poorly educated social network may not be capable of imparting the informational support needed to adhere to treatment and thereby control hypertension.51
Another explanation to the discrepancy of our results with other studies might be differences in individual and cultural characteristics. A large proportion of unemployed individuals may have skewed our sample towards a higher level of social support. People value financial support and therefore financially dependent individuals may report receiving high support. Also, the threshold for expected support may vary between different societies, for example in a patriarchal society like Nepal, women as primary care takers in the family may have a lower threshold of social support, whereas elderly men who command more respect in society may have a higher threshold.
We found a numerically higher prevalence of controlled hypertension among those receiving moderate support from friends but not those receiving higher support. A possible explanation might be that those receiving higher support spend longer time with friends and are thereby more exposed to peer pressure for unhealthy behaviour which was indicated as a barrier for effective control of blood pressure in our formative study in the same population.52 Reverse causation can also not be ruled out, as those with poorly controlled blood pressure may be receiving higher support from friends.
Strengths and Limitations
Our study adds to the sparse literature examining this association using validated instruments such as MSPSS and MMAS-8. We recruited hypertension patients from the community (not hospital) ensuring a representative sample. Since the outcome of interest (controlled hypertension and good adherence to antihypertensives) was common (larger than 10%), we fitted a modified Poisson regression model which gives a better approximation of the risk than overestimated odds ratio.53 This study is not without limitations. The cross-sectional design may have masked the true association between social support and controlled hypertension, as it is possible that individuals with uncontrolled hypertension or with poor adherence were receiving more support. Given the numerous statistical tests we conducted, it is essential to interpret any significant findings with caution to mitigate the risk of drawing false-positive conclusions. The findings are based on data from one urban municipality, which might limit the generalizability of our findings to the general hypertensive population in Nepal. Social support as a construct would be better explored using a mixed-method approach as the MSPSS tool does not capture the type of social support received.49 The reliance on self-reported data on medication and social support may have resulted in recall bias skewing the data in the direction of social desirability leading to over-estimated adherence and social support.
Conclusion
This study shows that hypertensive patients in Nepal in general have good social support.
However, social support was not foremost for medication adherence and control of hypertension. Future interventions for example digital technologies that facilitate remote monitoring and communication with care providers54 should nurture the high level of social support received by the hypertension patients. However, contextual studies to delineate the mechanisms through which social support can augment adherence to treatment, healthy behaviour, routine monitoring, and follow-up for hypertension management are needed for social support to have precedence in future interventions for hypertension patients.
Abbreviations
CVDs, Cardiovascular diseases; DAG, Directed acyclic graph; METs, Metabolic equivalents of task; MMAS, Morisky medication adherence scale; MSPSS, Multidimensional scale of perceived social support.
Data Sharing Statement
Data cannot be shared publicly for ethical reasons but are available on reasonable request to Ms Sanju Bhattarai and Dr Abhijit Sen.
Acknowledgments
We would like to thank all the participants in the study. We would like to thank field researchers Ms Apsara Basnet, Ms Geeta Tripathi, Ms Pema Tamang, Ms Prasoon Pandey, Mr Kishore Adhikari, Ms Sarita Bhandari, Ms Supriya Kharel.
The MMAS-8 Scale, content, name, and trademarks are protected by US copyright and trademark laws. Permission for use of the scale and its coding is required. A license agreement is available from MMAR, LLC., www.moriskyscale.com.
Funding
This work was supported by Norwegian University of Science and Technology, Trondheim, Norway (Project number 981023100).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Col Cardiol. 2017;70(1):1–25. doi:10.1016/j.jacc.2017.04.052
2. Lawes CM, Hoorn SV, Rodgers A. Global burden of blood-pressure-related disease, 2001. Lancet. 2008;371(9623):1513–1518. doi:10.1016/S0140-6736(08)60655-8
3. Chow CK. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA. 2013;310(9):959. doi:10.1001/jama.2013.184182
4. Bhattarai S, Aryal A, Pyakurel M, et al. Cardiovascular disease trends in Nepal – an analysis of global burden of disease data 2017. IJC Heart Vasculature. 2020;30(100602):100602. doi:10.1016/j.ijcha.2020.100602
5. Dhimal MBB, Bhattarai S. Report of non communicable disease risk factors: STEPS survey Nepal 2019. Kathmandu; 2020.
6. Collaborators NC, Stevens GA, Mathers CD. NCD countdown 2030: worldwide trends in non-communicable disease mortality and progress towards sustainable development goal target 3.4. Lancet. 2018;392(10152):1072–1088. doi:10.1016/S0140-6736(18)31992-5
7. Prevention, detection, evaluation, and treatment of high blood pressure the seventh report of the joint national committee on complete report. U.S. Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute, National High Blood Pressure Education Program; Contract No.: 04-5230; 2004.
8. Barth J, Schneider S, von Känel R. Lack of social support in the etiology and the prognosis of coronary heart disease: a systematic review and meta-analysis. Psychosomatic Med. 2010;72(3):229–238. doi:10.1097/PSY.0b013e3181d01611
9. Eom C-S, Shin DW, Kim SY, et al. Impact of perceived social support on the mental health and health-related quality of life in cancer patients: results from a nationwide, multicenter survey in South Korea. Psycho-Oncology. 2013;22(6):1283–1290. doi:10.1002/pon.3133
10. Tardy CH. Social support measurement. Am J Community Psychol. 1985;13(2):187–202. doi:10.1007/BF00905728
11. Scanfeld D, Scanfeld V, Larson EL. Dissemination of health information through social networks: twitter and antibiotics. Am J Infect Control. 2010;38(3):182–188. doi:10.1016/j.ajic.2009.11.004
12. Perry BL, Pescosolido BA. Functional specificity in discussion networks: the influence of general and problem-specific networks on health outcomes. Social Networks. 2010;32(4):345–357. doi:10.1016/j.socnet.2010.06.005
13. DiMatteo MR. Social support and patient adherence to medical treatment: a meta-analysis. Health Psychol. 2004;23(2):207–218. doi:10.1037/0278-6133.23.2.207
14. Trivedi RB, Ayotte B, Edelman D, Bosworth HB. The association of emotional well-being and marital status with treatment adherence among patients with hypertension. J Behavl Med. 2008;31(6):489–497. doi:10.1007/s10865-008-9173-4
15. Cornwell EY, Waite LJ. Social network resources and management of hypertension. J Health Social Behav. 2012;53(2):215–231. doi:10.1177/0022146512446832
16. Gallant MP, Spitze GD, Prohaska TR. Help or hindrance? How family and friends influence chronic illness self-management among older adults. Research on Aging. 2007;29(5):375–409. doi:10.1177/0164027507303169
17. Callaghan P, Morrissey J. Social support and health: a review. J Adv Nurs. 1993;18(2):203–210. doi:10.1046/j.1365-2648.1993.18020203.x
18. Bolger N, Zuckerman A, Kessler RC. Invisible support and adjustment to stress. J Pers Soc Psychol. 2000;79(6):953–961. doi:10.1037/0022-3514.79.6.953
19. Norris FH, Kaniasty K. Received and perceived social support in times of stress: a test of the social support deterioration deterrence model. J Pers Soc Psychol. 1996;71(3):498–511. doi:10.1037/0022-3514.71.3.498
20. Idler EL, Boulifard DA, Contrada RJ. Mending broken hearts. J Health Social Behav. 2012;53(1):33–49. doi:10.1177/0022146511432342
21. Ford CD, Sims M, Higginbotham JC, et al. Psychosocial factors are associated with blood pressure progression among African Americans in the Jackson Heart Study. Am J Hypertens. 2016;29(8):913–924. doi:10.1093/ajh/hpw013
22. Taher M, Abredari H, Karimy M, Abedi A, Shamsizadeh M. The relation between social support and adherence to the treatment of hypertension. J Educ Community Health. 2014;1(3):63–69. doi:10.20286/jech-010348
23. Padhy M, Lalnuntluangi R, Chelli K, Padiri RA. Social support and adherence among hypertensive patients. AJHM. 2016;1(1):33–40.
24. Pan J, Hu B, Wu L, Li Y. The effect of social support on treatment adherence in hypertension in China. Patient Preference Adherence. 2021;15:1953–1961. doi:10.2147/PPA.S325793
25. Osamor PE. Social support and management of hypertension in south-west Nigeria: cardiovascular topic. Cardiovasc J Afr. 2015;26(1):29–33. doi:10.5830/CVJA-2014-066
26. Sabaté E, World Health O. Adherence to long-term therapies: evidence for action. World Health Organization. 2003;194.
27. Adisa R, Olajide OO, Fakeye TO. Social support, treatment adherence and outcome among hypertensive and Type 2 diabetes patients in ambulatory care settings in southwestern Nigeria. Ghana Med J. 2017;51(2):64–77.
28. Hm ST, Quyyumi A, Reilly C, Pemu P, Dunbar S, Dunbar S. The relationship among health beliefs, depressive symptoms, medication adherence, and social support in African Americans with hypertension. J Cardiovasc Nurs. 2019;34(1):44–51. doi:10.1097/JCN.0000000000000519
29. Uchino BN. Understanding the links between social support and physical health: a life-span perspective with emphasis on the separability of perceived and received support. Perspectives Psychol Sci. 2009;4(3):236–255. doi:10.1111/j.1745-6924.2009.01122.x
30. Acharya R, Chaudhary A, Pandey J, Pandey C. Self-Care Management And Its Associated Factors Among Patient With hypertension in Nepal. J Chitwan Med Coll. 2022;12(2):91–96. doi:10.54530/jcmc.637
31. Karki M Budhanilakantha municipality profile; 2019.
32. Bhattarai S, Shrestha A, Skovlund E, Åsvold BO, Mjølstad BP, Sen A. Cluster randomised trial to evaluate comprehensive approach to hypertension management in Nepal: a study protocol. BMJ open. 2023;13(5):e069898. doi:10.1136/bmjopen-2022-069898
33. Morisky DE AA, Krousel-Wood M, Ward HJ, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348–354. doi:10.1111/j.1751-7176.2008.07572.x
34. De M Concurrent and predictive validity of a self-reported measure of medication adherence; 1986.
35. Lee GKY, Wang HHX, Liu KQL, Cheung L, Morisky DE, Wong MCS. Determinants of medication adherence to antihypertensive medications among a Chinese population using morisky medication adherence scale. PLoS One. 2013;8(4):e62775. doi:10.1371/journal.pone.0062775
36. Stewart RC, Umar E, Tomenson B, Creed F. Validation of the multi-dimensional scale of perceived social support (MSPSS) and the relationship between social support, intimate partner violence and antenatal depression in Malawi. BMC Psychiatry. 2014;14(1). doi:10.1186/1471-244X-14-180
38. Global physical activity questionnaire Global Physical Activity Questionnaire (GPAQ). [Internet]. Available from: www.who.int/chp/steps. Accessed March 21, 2024.
39. World Health Organization. GLobal status report on non communicable diseases 2014; 2014.
40. Textor J. Adjustment criteria in causal diagrams: an algorithmic perspective. In Proceedings of the 27th Conference on Uncertainty in Artificial Intelligence (UAI 2011) [press release]; 2011.
41. StataCorp. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC; 2023.
42. Ademe SAF, Gela D, Gela D. Hypertension self-care practice and associated factors among patients in public health facilities of Dessie town, Ethiopia. BMC Health Serv Res. 2019;19(1):1–10. doi:10.1186/s12913-019-3880-0
43. Rabia Hacihasanoglu Asilar AY, Saglam R, Demirturk Selcuk E, Erduran Y, Sarihan O. The effect of loneliness and perceived social support on medication adherence self-efficacy in hypertensive patients: an example of Turkey. Eur J Cardiovasc Nurs. 2020;38(4):183–190.
44. Nur Syafaah Nazeri NM, Redzuan M, Abdul Mulud Z. Social support and self-care practice among patients with hypertension in a teaching hospital. Malaysian J Med Health Sci. 2021;18(8):281–290.
45. Redondo-Sendino PG-C Á, José RB, Rodríguez-Artalejo F, Rodríguez-Artalejo F. Relationship between social network and hypertension in older people in Spain. Rev Esp Cardiol. 2005;58(11):1294–1301.
46. Jiwon Baek NWH, Chang Kim H, Youm Y, Youm Y. Sex-specific effects of social networks on the prevalence, awareness, and control of hypertension among older Korean adults. J Geriatric Cardiol. 2016;13(7):580–586. doi:10.11909/j.issn.1671-5411.2016.07.005
47. Luu Quang Thuy NHT, Hong Trung L, Huy Tan P, et al. Blood pressure control and associations with social support among hypertensive outpatients in a developing country. Biomed Res Int. 2021;2021:1–10.
48. Bingjie Shen TG, Xinyu D, Chenyang P, Zhao J, Liu Y, Liu Y. Medication adherence and perceived social support of hypertensive patients in China: a community-based survey study. Patient Preference Adherence. 2022;16:1257–1268. doi:10.2147/PPA.S363148
49. Hatah ELK, Ali AM, Mohamed Shah N, Islahudin F, Islahudin F. The influence of cultural and religious orientations on social support and its potential impact on medication adherence. Patient Prefer Adherence. 2015;9:589–596. doi:10.2147/PPA.S79477
50. Acharya TDG, Traille K, Dhakal H. Senior citizens in Nepal: policy gaps and recommendations. Gerontol Geriatr Med. 2023;9:23337214231179902.
51. Isa MD, Shahar SHF, He FJ, Majid HA. Associations of health literacy with blood pressure and dietary salt intake among adults: a systematic review. Nutrients. 2021;13(12):4534.
52. Bhattarai S, Bajracharya S, Shrestha A, et al. Facilitators and barriers to hypertension management in urban Nepal: findings from a qualitative study. Open Heart. 2023;10(2):e002394. doi:10.1136/openhrt-2023-002394
53. Spiegelman D. Easy SAS calculations for risk or prevalence ratios and differences. Am J Epidemiol. 2005;162(3):199–200.
54. Kario K, Nomura A, Harada N, et al. Efficacy of a digital therapeutics system in the management of essential hypertension: the HERB-DH1 pivotal trial. Eur Heart J. 2021;42(40):4111–4122. doi:10.1093/eurheartj/ehab559
‘Global Africa” is a term popularised by the late Kenyan scholar Ali Mazrui and used to refer to African diasporas of enslavement and colonialism, covering the Americas, the Caribbean, Europe and the Indian Ocean.
My recently publishedGlobal Africa: Profiles in Courage, Creativity and Cruelty (Jacana) consists of 100 essays, written over the past three post-apartheid decades. They cover historical and political figures, technocrats, activists, writers, public intellectuals, music and film artists and sporting figures.
The essays seek to capture the zeitgeist of the post-apartheid era, arguing that Africa’s liberation struggles were mirrored by similar anti-colonial battles in the Caribbean as well as the American civil rights movement.
The book examines three historical figures: Cecil Rhodes, Mahatma Gandhi and Woodrow Wilson.
Rhodes was the greatest symbol of imperialism during the late 19th century, plundering Africa’s riches by often brutal means while expanding British colonial territory.
Wilson was the US president from 1913 to 1921. His supposedly “liberal” foreign policy entailed imperial “gunboat diplomacy” in Latin America and the Caribbean.
Gandhi has been widely lauded for his role in the liberation of the colonial world. His many racist utterances during his 21 years in South Africa (1893-1914) have, however, recently tarnished his legacy in Africa and beyond.
The book also provides kaleidoscopic profiles of 18 African and eight Western political figures: Ghana’s Kwame Nkrumah and two of South Africa’s Nobel peace laureates, Albert Luthuli and Nelson Mandela, as well as Thabo Mbeki, were all actively involved in Africa’s liberation movement as Prophets of the Pan-African Pantheon.
Mbeki was the heir of Nkrumah, with both acting as philosopher-kings seeking to craft a visionary pan-African foreign policy. Zambia’s Kenneth Kaunda and Zimbabwe’s Robert Mugabe both contributed greatly to the liberation of southern Africa, but instituted autocratic rule and oversaw catastrophic economic policies. FW de Klerk ruled an undemocratic apartheid state, but embarked on peacemaking with fellow Nobel laureate, Mandela, to usher in democratic rule.
Nigeria’s Olusegun Obasanjo and Ghana’s Jerry Rawlings were autocratic military rulers before becoming elected civilians, though Rawlings remained more popular among his citizens.
South Africa’s Jacob Zuma – dogged by allegations of graft – had a similar cunning “native intelligence” to Obasanjo’s, while controversial Nobel peace laureate, Liberian president Ellen Johnson Sirleaf (who had funded Liberian warlord Charles Taylor during the country’s civil war in the 1990s), was a technocrat politician.
Ethiopia’s Meles Zenawi and Nobel peace laureate Abiy Ahmed both ruled as strong-fisted, intellectual freedom fighters. Zaire’s Western-backed Mobutu Sese Seko’s 31-year rule brought about the very chaos he had repeatedly argued that only he could prevent.
Uganda’s Idi Amin and Kenya’s Daniel arap Moi oversaw tyrannical regimes, mirrored by Rwanda’s Paul Kagame. Libya’s mercurial Muammar Gaddafi suffered from monarchical delusions of grandeur, while promoting a quixotic pan-Africanism.
US Democratic presidents – Bill Clinton and Kenyan-Kansan Nobel peace laureate Barack Obama – were both intelligent, charismatic but ultimately cynical leaders who, respectively, oversaw the forced withdrawal of UN peacekeepers from Rwanda at the height of the 1994 genocide, and the extended militarisation of Africa by the US military in the 2010s.
American president Donald Trump, British prime ministers Margaret Thatcher, Tony Blair and Boris Johnson, and French president Nicolas Sarkozy all expressed prejudiced thinking towards Africa. The legacies of two US secretaries of state – Colin Powell and Madeleine Albright – are also assessed.
The perspectives, personalities and performance of 14 global technocrats are then examined: Egypt’s Boutros Boutros-Ghali; Ghana’s Nobel peace laureate Kofi Annan; Nigeria’s Adebayo Adedeji, Ibrahim Gambari, Margaret Vogt, Ngozi Okonjo-Iweala and Eloho Otobo; Algeria’s Lakhdar Brahimi; Tanzania’s Augustine Mahiga; South Africa’s Nkosazana Dlamini Zuma, Naledi Pandor and Mamphela Ramphele; Argentina’s Raúl Prebisch; and France’s Jean Monnet.
I then turn to the legacies of seven activists from Global Africa: American civil rights stalwarts, Nobel peace laureate Martin Luther King Jr and John Lewis; Kenyan environmental campaigner Wangari Maathai and her Congolese fellow Nobel laureate, anti-sexual violence campaigner Denis Mukwege (who unsuccessfully ran for his country’s presidency last year); martyred Nigerian environmental activist Ken Saro-Wiwa; and two martyred South Africans, Ruth First and Solomon Mahlangu.
Two Europeans are highlighted who contributed to Africa’s political (Tor Sellström) and journalistic (Kaye Whiteman) struggles.
I then analyse the rich diversity of African literature, starting with the influence of 19th-century British writer Charles Dickens on the continent’s writers, before profiling Nigeria’s Chinua Achebe, Nobel laureate Wole Soyinka, Buchi Emecheta and John Pepper Clark, as well as America’s James Baldwin, Maya Angelou, Nobel laureate Toni Morrison and bell hooks.
Ten public intellectuals are then showcased who pioneered Africa’s Triple Heritage (Kenya’s Ali Mazrui); Post-Colonial Studies (Palestinian American Edward Said); Négritude Literary Criticism (Nigeria’s Abiola Irele); Post-Colonial African Literary Criticism (Kenya’s Chris Wanjala); the Political Economy of Rebel Movements in Africa (Malawian-Swede Thandika Mkandawire); the Politics of Rural Societies in Africa (Nigeria’s Raufu Mustapha); America’s Prison Industrial Complex (African-American Angela Davis); and the Struggles for Global Reparations (America’s Randall Robinson, Barbadian Hilary Beckles and Nigeria’s Ade Ajayi).
I examine the legacies of seven artistes: Iconoclastic, anti-establishment rebels, Nigeria’s Fela Aníkúlápó Kuti and Jamaica’s Bob Marley; American multiple Grammy-winning superstar Michael Jackson; Bahamian American Oscar-winning actor Sidney Poitier; Nigerian-British Oscar-nominated actress Cynthia Erivo; and Nigerian Grammy-winning Burna Boy and his songbird compatriot, Asa.
I conclude by assessing the legacies of 21 of the greatest sporting figures in history: Three-time African-American world boxing heavyweight champion and civil rights campaigner Muhammad Ali; Afro-Brazilian three-time World Cup winner Pelé; Mozambican-born European footballer of the year Eusébio; Argentinian World Cup-winning captain Diego Maradona; Africa’s only Ballon d’Or winner, Liberia’s George Weah; five African players of the year: Cameroon’s Samuel Eto’o, Ivorian Didier Drogba, Egypt’s Mohamed Salah, Senegal’s Sadio Mané and Gabon’s Pierre-Emerick Aubameyang; the all-conquering anti-apartheid West Indian cricket team of Viv Richards, Clive Lloyd, Michael Holding and Joel Garner; American quadruple Olympic gold medal sprinter Jesse Owens; rugby’s first global superstar, New Zealand’s Jonah Lomu; Spanish tennis phenomenon Rafael Nadal; Nigerian American two-time NBA (National Basketball Association) champion Hakeem Olajuwon; and my late businessman father and sports administrator Israel Adebajo.
With negative stereotyping and widespread Afrophobic views of the continent and its diaspora still so rife in the Western imagination and media, it is critical to counter these views through these giants of Global Africa. DM
ABCD Africa is proud to announce the release of the 2nd edition of the 100 Most Impactful Voices List to mark 2024 International Women’s Day. This list recognizes African female coaches, content creators, and community builders who leverage their voices and digital content as tools for impact.
In a world grappling with unprecedented challenges ranging from climate crises to systemic injustices, the voices of women are more crucial than ever.
Through the 100 Most Impactful Voices list, we shine a spotlight on women who harness the power of digital platforms to address these pressing issues head-on.
They are the architects of transformation, leveraging their voices to dismantle barriers, challenge norms, and uplift communities across various digital platforms, including Instagram, Twitter, Facebook, YouTube, LinkedIn, TikTok, Netflix, Podcasts and Blogs.
“We are thrilled to unveil the 100 Most Impactful Voices in Africa and amplify their contribution. We hope that this list inspires other women to use their voices, create impactful content, and shape conversations that contribute to the development of a more equitable and inclusive society,’’ says Joke Pearl Oyebamiji, Founder of ABCD Africa.
The selection process was rigorous and thorough, with nominations received from digital experts and the general public. The finalists were evaluated based on their creativity, impact, authenticity, and engagement.
Here they are (This list is in no particular order):
Economic and Human Capital Policy Expert, Good Governance Champion
Dr. Oby Ezekwesili is an eminent figure in Nigeria, renowned for her expertise in economic policy, advocacy for transparency, and commitment to good governance and human capital development. A former vice president at the World Bank, she has championed initiatives like #BringBackOurGirls, lending her voice to pressing issues and driving crucial conversations through her social media platforms where she has over 1.4 million followers.
Yemisi Adegoke, a former CNN Africa journalist and current BBC Africa reporter, has garnered acclaim for her incisive journalism. With a focus on addressing misinformation, she engages audiences with thought-provoking storytelling that raises awareness and sparks dialogue about pressing issues in Africa.
Dr. Addy Olubamiji, is the CEO of D-Tech Centric Ltd. and Founder of STEMHub Foundation Canada, where she champions STEM education and empowerment for youths and immigrants through training programs and digital content.
A Nigerian-American technologist and pioneer in metal and plastic additive manufacturing, she broke barriers by becoming the first Black person to obtain a PhD in Biomedical Engineering from the University of Saskatchewan.
Nozipho Tshabalala, a renowned conversation strategist and award-winning financial markets broadcaster, excels in moderating global conversations for measurable outcomes. With courage and insight, she navigates difficult discussions for leading global institutions, listed multinational corporations, and civil society organizations.
As an executive director at LRMG and a faculty member for Duke Corporate Education, Nozipho is committed to leveraging conversations for transformative change in Africa and beyond.
Stella Ndekile, a visionary serial entrepreneur, host of « Walk with Stella » show, and author of “Success Uncharted,” leads Nuban Beauty Ltd, a premier cosmetic brand catering to African skin tones.
With over a decade of experience in business development and cosmetics, Stella empowers individuals to feel confident through her premium beauty products and impactful digital content.
Chinyere Okorocha, Chairperson of the Nigerian Bar Association Women Forum, is a distinguished IP and medico-legal lawyer.
Passionate about empowering female professionals, she founded the Heels & Ladders Career Mentorship Club, providing invaluable guidance for career advancement through her digital content and programs.
Fatma Said Kauga is the visionary Founder and Executive Director of Doyenne Organization, dedicated to nurturing the next generation of female leaders in Tanzania.
Recognized as a Gratitude Network Fellow and a Perennial Leadership Fellow, Fatma is committed to empowering youth and women to drive sustainable change through various initiatives and digital content.
Esther Ijewere, a renowned media strategist and author, is the Founder of Women of Rubies, championing women’s rights and empowerment. Recognized for her impactful advocacy, Esther’s work has earned prestigious awards and accolades, including the Women Enterprise Award from Vital Voices International.
Through her platforms and initiatives, Esther inspires positive change and celebrates individuals making a difference.
Nana Agyemang is a multimedia journalist, creative strategist, and writer known for her impactful work with The Cut, Refinery29, ELLE Magazine, New York Times, and BBC News.
As the founder of EveryStylishGirl, she champions diversity and empowerment in fashion and media, creating a vibrant community that amplifies the voices of women of color and advances opportunities in the industry.
Int’l Board Certified Lifestyle Medicine Physician
Dr. Chinasa Amadi, a Russian-trained Medical Doctor and Board Certified Lifestyle Medicine Physician, champions holistic healthcare in Africa.
Founder of Ariella Health and Fitness Ltd, she empowers communities through Africa’s first Digital Lifestyle Medicine Practice, offering CPD accredited health coaching courses and reaching thousands worldwide with her digital content.
Producer & Documentary Filmmaker at StoryTeller Media Global
Toyin Poju-Oyemade is a seasoned media professional with over 16 years of experience spanning radio, television, and documentary filmmaking.
As the founder of StoryTeller Media, she is dedicated to curating powerful conversations and showcasing the journeys of everyday people. With a passion for storytelling, Toyin has collaborated with various organizations, producing qualitative documentaries that inspire and resonate.
Founder – Northern Hibiscus Community, Chairperson – Falke Group of Companies
Aisha Falke is a serial entrepreneur and visionary leader dedicated to empowering Northern Nigerian women and youth. As the Founder of Northern Hibiscus Community which has over half a million followers, she leverages her passion for storytelling and community building to drive positive change.
Through initiatives like the Northern Youth Summit and Edu-Kids Academy, she strives to tackle poverty and educational challenges in Northern Nigeria.
Lynn Ngugi, an award-winning journalist and YouTuber, is renowned for her captivating coverage of human interest and societal issues.
Transitioning from her role at Tuko to her self-titled YouTube show which has amassed over 850,000 subscribers, Lynn has garnered international acclaim for her impactful storytelling.
Recognized with prestigious awards like the BEFFTA Best International Media Personality and the Gender Justice Champion Award, she continues to inspire change through her advocacy.
Adedayo Tosin Olufemi, the visionary founder of Newmumshub.com, passionately advocates for new mothers through her online platform which boasts of over 130,000 followers.
New Mums Hub serves as a nurturing community, offering support and guidance to mothers embarking on the journey of motherhood.
Reni Odetoyinbo, a Canadian-Nigerian blogger, empowers women worldwide through her transformative resources on financial literacy and lifestyle tips.
Recognized by YouTube as part of the prestigious #YouTubeBlack Voices Class of 2022, Reni’s engaging video content inspires women to take control of their financial futures and pursue their professional aspirations.
Iquo Ukoh, a Nigerian food expert, consultant, and podcaster, celebrates the richness of Nigerian cuisine through her blog, 1Q Food Platter. Her cookbook, “Memories on a Platter,” documents her culinary journey and promotes Nigerian identity through food.
Iquo’s irresistible presentations and delicious recipes educate and inspire food lovers while reflecting her commitment to preserving Nigerian culture.
Founder – Afrique Femme, Founder – Yelenba Women in Action
Aissata Sidibe N’Dia is the President and founding member of Yelenba-Women in Action, an NGO dedicated to empowering women and raising awareness among young girls in Ivory Coast.
With over 18 years of experience in communications and an MBA from the University of Maryland, USA, she founded the Afrique Femme platform, which has over 150,000 followers. Aissata champions African women leaders through her show, African Woman 2.0.
Chinny Ononuju-McErnest is the Founder of The Women International (TWI), where she leads a global movement empowering women through various initiatives and digital content across multiple countries.
Chinny’s marketing expertise, showcased at W Agency, is utilized to amplify the impact of renowned foundations and NGOs, driving societal change.
Ogheneyonreme Karika is a Networking and People Strategy Expert. Karika educates thousands of entrepreneurs and professionals globally through her social media platforms on personal branding and networking, accelerating their careers and business visibility.
Ife Durosinmi-Etti, founder of Herconomy, is dedicated to empowering women in business through funding, mentorship, training programs, and impactful digital content.
Herconomy provides a platform for women to connect, save money, and access opportunities, aiming to address the challenges of funding and self-development faced by women.
Ife’s passion for women’s empowerment has led to impactful initiatives and partnerships with global organizations like Amazon and Google.
Arian Simone is the Co-Founder and General Partner of Fearless Fund, the first VC fund by women of colour for women of colour. With over 17 years of entrepreneurial experience, she pioneers initiatives supporting Black women entrepreneurs.
Despite legal opposition, her work in economic empowerment and advocacy uplifts underrepresented founders, challenging systemic barriers to diversity, inclusion and economic empowerment.
Victoria James, known as Veekee James, is an award-winning fashion designer, content creator, and social media influencer. Her brand, Veekee James, inspires creativity and elegance globally with unique, custom-crafted pieces.
With over 1 million Instagram followers, she shares her faith through her gospel podcast – Bible Stories With VJ.
Recipe Developer, Founder – Atarefoods, Lose It Nigerian, Jollof Code
Ronke Edoho, a Nigerian-born Chartered Accountant and certified nutritionist, is the culinary genius behind 9jafoodie. Through her platform, Ronke celebrates Nigerian cuisine while promoting wellness through nutrition.
Her blog offers authentic recipes, cooking tips, and nutritional insights, empowering her audience to make healthier food choices and embrace the richness of Nigerian food culture.
Joycee Awosika is a visionary entrepreneur known for building impactful global companies in wellness, manufacturing, and tech sectors. As Founder of ORiKi Group, she has expanded wellness spas across Africa.
Leveraging her expertise, impactful digital content, and transformative programs, she empowers entrepreneurs with systems, structure and faith-based advisory.
Featured in CNN, CNBC, and Ebony Magazine, Joycee’s leadership inspires women worldwide.
Hayet Rida, a Ghanaian-born entrepreneur and influencer, is known for her resilience and creativity in the fashion and lifestyle industry. From founding luxury candle brand AÏYA CANDLE CO to launching her jewelry line, KHOI Studio, she’s a master of pivoting failures into success.
With a passion for empowering others, Hayet shares her life experiences openly, inspiring her followers to embrace confidence and self-love.
Haoma Worgwu is an award-winning thought leader and LinkedIn expert, renowned for helping business owners and professionals maximize opportunities on the platform. Her impactful digital programs, including the “20 Days LinkedIn Growth Program,” have impacted thousands globally.
Recognized as one of the top LinkedIn creators in Nigeria, Haoma’s influence extends to global forums, earning her accolades from the United Nations and Goldman Sachs.
Dr. Tewa Onasanya, a British-Nigerian philanthropist, publisher and mindset stylist, is the visionary behind Exquisite Magazine and the ELOY Awards.
Through her platforms, initiatives and digital content, she celebrates excellence in fashion, beauty, and entertainment while promoting empowerment and self-confidence.
Claudia Lumor, founder and editor-in-chief of Glitz Africa, has transformed the fashion landscape in West Africa through her influential lifestyle publication. As a UN (UNFPA) Ambassador for Ghana, Claudia is dedicated to promoting and telling inspiring African stories. Her innovative work has earned her numerous awards and accolades.
Sola Adesakin is a seasoned finance coach and chartered accountant. Through Smart Stewards Financial Advisory Limited in Nigeria and the USA, she has transformed lives financially across 40 countries, guiding people from financial stress to rest, from debt to wealth, and from mediocrity to an extraordinary life.
Claire Idera Nnani is a versatile artist known for her delicate portrayals of the transformative journey of young black women. Her work, inspired by personal journals and introspection, explores themes of identity and growth through whimsical elements and vibrant colors.
With a background in architecture and fashion design, Claire also shares her creative expertise through teaching and authentic lifestyle content on her YouTube channel where she has amassed over 52,000 subscribers.
Candy Olatunji, a Certified Health Coach and Weight Management Expert, transforms lives by providing tailored guidance on maintaining a healthy lifestyle.
With over half a million followers across digital platforms, Candy educates on calories, metabolism, and simple fitness routines through ebooks and personalized coaching sessions.
Hannah Kupoluyi, founder and CEO of All Women’s Network, is a multi-award-winning business coach and advocate for women’s empowerment.
Through transformative initiatives like Discover Your Business Spark workshops, she empowers women to overcome challenges and thrive in business.
Hannah’s strategic use of impactful content, coupled with her dedication to women’s advancement, has earned her recognition as a UN Women delegate and numerous prestigious awards.
Social Entrepreneur, Founder – Africa Creative Market Global
Inya Lawal is a social entrepreneur and founder of Ascend Studios Foundation and the Africa Children’s Creative Network, dedicated to empowering women, youth, and nurturing creative skills in children.
She leads Ascend Studios, producing impactful TV and feature content while consulting for brands. Inya’s leadership extends to international programs, board memberships, and receiving honors for her contributions to women’s leadership and global trade development.
Olabisi Adamu, founder of Ignite Nations Ministry, is a Prophet, Intercessor, and seasoned teacher of God’s word. With a passion for spiritual growth and business empowerment, she leads thousands in prayer daily and owns Pro Thirty One Designs, an interior design showroom in Abuja.
Through her ministry, businesses, digital content, and philanthropic initiatives, Olabisi ignites individuals to excel spiritually and prosper in all aspects of life.
Solafunmi Oyeneye is a seasoned Media, Tech, and Entertainment Executive with over 15 years of experience. Passionate about financial empowerment, Solafunmi runs Wealth Motley, a platform dedicated to teaching financial literacy and wealth creation, reaching over 75,000 individuals.
As the VP of Business & Strategic Partnerships at Circo, she drives innovation in African storytelling.
Titoluwa Sam-Oladapo, known as Titothewriter, is a writer, culture shaper, and advocate breaking the silence on vaginismus through her book “Pop My Cherry Now.” She shares her journey of living with and overcoming vaginismus, addressing stigma and sexual assault.
Through her Instagram and YouTube, Tito discusses faith-led Christianity, emphasizing grace over condemnation and shattering sexual stigma in the gospel and society.
Pretty Amagbakhen, a licensed mental health therapist and ADHD coach, courageously addresses mental health issues and dismantles stigma. With empathy and intuition, she offers invaluable support through her social media content, fostering a safe space for her audience to thrive.
Yacine Diop Djibo, Founder of Speak Up Africa, is a leading voice in Africa’s public health landscape. Since 2011, her organization has tackled issues like malaria and sanitation, fostering collaboration with African leaders.
Yacine’s influence extends to multiple boards, including the RBM Partnership to End Malaria.
Sola Allyson-Obaniyi, known as Shola Allyson, is a renowned Nigerian soul and folk singer-songwriter. She’s a voice coach and consultant, sharing her vulnerability and soulful storytelling to inspire personal growth and spiritual reflection.
Her music, including hits like “Eji Owuro” and “Obinrin Ni Mi,” blends traditional Yoruba folk with contemporary gospel.
Bolatito Bez-Idakula, known as Tito, is the Founder of My Lighthouse, a faith-based blog. With a background in banking and a passion for sharing God’s love, she writes on self-identity, self-love, and honest motherhood stories.
Through vulnerable narratives on social media, Tito aims to inspire healing, encourage deeper spiritual connections, and empower others to live their best lives.
Adetoke Oluwo is a dynamic TV producer, screenwriter, and Creative Director of the renowned Ankara ready-to-wear fashion brand, Sgtcclothing. From covering international fashion events to training entrepreneurs, Adetoke’s journey reflects her passion for both fashion and business.
Through her Instagram page where she reaches over 67,000 followers, she shares daily tips to uplift and empower others, while unashamedly expressing her love for Jesus.
High-Performance Coach, Founder & CEO – DCG Consulting Group
Dizigbordi Kwaku is a seasoned Business Leader with nearly three decades of experience in corporate America and Africa. As the Founder and Chief Strategist of The DCG Consulting Group, she specializes in personal development, professional growth, and talent development.
Through her professional work, training programs, and digital content, Dizigbordi is dedicated to empowering individuals and organizations to reach their full potential.
Maryam O. Belgore is a dedicated advocate for Youth & Girls Empowerment in Nigeria. Through her NGO, the Maryam Onikijipa Belgore Foundation, she tirelessly works to improve the lives of underprivileged youths & girls by providing access to education and essential supplies.
Through her talk-show, “Unraveling with Maryam,” she shares insights on life and gratitude.
Hauwa Ojeifo is a trailblazing advocate for mental health awareness and women’s rights in Nigeria. As the Executive Director of She Writes Woman, she empowers individuals with lived mental health experiences to share their stories, co-create solutions, and advocate for their rights.
Hauwa’s groundbreaking work has garnered international recognition, including prestigious awards from organizations like the Queen’s Young Leaders and the Bill and Melinda Gates Foundation.
Oluseye Yemisi Aderonke, fondly called DIBIA, is a Certified Holistic Nutrition Practitioner, Health Coach, and Naturopath. As the founder and CEO of FD Naturales & Essential Oils Ltd, she inspires wholeness in individuals through holistic health and wellness practices.
With a passion for natural alternatives, she has helped thousands regain their health through educational posts, holistic programs, and her authored books.
Speaker, Founder – Nala Feminist Collective, I Am Nala Podcast
Aya Chebbi, a Tunisian diplomat and passionate pan-African feminist activist, made history as the youngest senior official in the African Union’s history.
Through various initiatives, storytelling and her podcast – I am Nala, she advocates for youth empowerment and the advancement of women’s rights.
Commercial Director, Founder – Uncommon Woman Movement
Ifeoma Chuks-Adizue is a seasoned leader with over 18 years of experience driving growth in people and organizations across Africa.
As the Founder of the Uncommon Woman Movement, she empowers black career women to unleash their potential, achieve career success, and create impactful businesses through her transformative programs and digital content.
Habibah Waziri, a seasoned Human Capital Strategist and Business Solutions expert with nearly a decade of experience regularly shares her expertise through digital content, panels, keynotes, and workshops globally.
As the Managing Director/CEO of BGR Consulting Ltd, she implements human capital development programs and business growth strategies across Africa.
Irene Kiwia is a seasoned entrepreneur with over 17 years of experience in media, marketing communications, and technology. As the Founder of Adanian Labs, Twaa, eCOBbA, and The Africa Blockchain Center, she is dedicated to empowering women and youth across Africa.
Irene’s innovative digital content & impact tech platforms aim to provide access to finance, communities, and capacity building, driving wealth creation for women in Africa.
Blessing Oyeleye Adesiyan is a leading voice, recognized for her pioneering work in building robust care infrastructure for today’s workforce. As the Founder & CEO of Mother Honestly and Caring Africa, she leads initiatives aimed at advancing workplace equity globally through her programs, offerings, and digital content.
Yeside Olayinka-Agbola, also known as ‘Olori Coitus,’ is a certified sexual and reproductive health educator and intimacy expert. Through her enterprise, Olori Coitus, she challenges taboos around sex in Nigeria, providing sexual health education and coaching to individuals and couples.
As the host of the Olori Coitus Podcast, she explores relationships, sex, pleasure, and intimacy, empowering listeners with knowledge they wish they had growing up.
Mariéme Jamme, a Senegalese-born French-British Technologist and Young Global Leader, is the CEO of Spotone Global Solutions and founder of iamtheCODE.
Through iamtheCODE, she mobilizes global support to empower 1 million girls in STEAMD education by 2030.
Mariéme’s inspirational podcast and Instagram series blend Japanese and African philosophies to bring joy and purpose to her audience, while her advocacy for marginalized communities resonates worldwide.
Ndidi Nwuneli is an expert on African agriculture, entrepreneurship, and youth development. As the co-founder of AACE Foods & Sahel Consulting, she works to improve nutrition in Africa. Recognized globally, she serves on several boards and is committed to changing narratives about Africa through food.
Uche Pedro is the visionary founder of BellaNaija, Africa’s foremost lifestyle and advocacy digital media company. With over 12 million active users, BellaNaija has revolutionized creative industries across Africa.
Uche’s influence extends beyond media, as she champions positive change through initiatives like #BNDoGood. Recognized as one of Africa’s most powerful women by Forbes, Uche is dedicated to fostering progress for Africa’s emerging generations.
Rorisang “Rori” Thandekiso is a versatile South African talent, renowned as an actress, musician, and presenter. As the lead vocalist of MuzArt and a former YOTV presenter, she has left an indelible mark on South Africa’s entertainment landscape.
With acting roles in popular TV shows, hosting gigs on prominent platforms like Mzansi Insider, and her digital content, Rori engages her over 400,000 followers with her bubbly personality and unwavering dedication to youth advocacy.
Temilade Salami Olanrewaju is a Climate Education and Communications Expert, dedicated to driving environmental change in Nigeria. As the Executive Director of “EcoChampions”, she leads initiatives in climate education, tree planting, and plastic waste management.
Through her digital content, books and poetry, she creatively advocates for environmental consciousness and self realization.
Bola Matel-Okoh is a seasoned attorney and Non-Executive Director with over 30 years of legal experience. As the Lead Coach and Founder of BMO Advisory Services and The Women’s Lifestyle Hub, she empowers executive women to achieve personal and professional excellence.
Through her transformational programs and digital content, she guides women to unlock their full potential.
Entle Mmipi is the founder of Finpowerment Botswana, which aims to impact the youth with financial literacy and entrepreneurship skills through age-appropriate and interactive methods, as a way to assist in alleviating poverty and unemployment in Botswana.
Banke Fasominu is the CEO and Creative Director of Oludidit, a renowned creative enterprise specializing in arts and crafts. With a passion for blending African and Western elements, she transforms imaginations into tangible products, from interior decor accessories to stationeries.
Banke also shares her wisdom through her video series “Dear Young Lady,” offering authentic life advice distilled from her own experiences.
Dr. Yetunde A. Omede, Ph.D., is a professor at Farmingdale State College and Director of Community and Civic Engagement. A Fulbright Specialist Scholar, she champions good governance and global ethics.
Her work spans academia, policymaking, and humanitarian efforts, earning her numerous awards, including induction into Rutgers University’s African-American Hall of Fame. As a global speaker and author, Dr. Yetunde empowers youth and women worldwide to effect positive change.
Hilary Rodriguez-Taiwo, a Nigerian Cosmetic Scientist, brings science to skincare. With a BSc in Cosmetic Science, she’s formulated for Procter and Gamble and consulted for brands like Lancôme and Chanel.
As founder of Hilary Says, she champions quality beauty products for all skin types. Her platform offers research-driven advice, empowering individuals to make informed skin care choices.
Mariama Khai Fornah is a seasoned journalist, gender activist, and visionary leader. With over 18 years of experience, she has reported on significant events, including the trials of former President Charles Taylor in The Hague.
As CEO of Hands of Hope Radio 100.5 FM, Sierra Leone’s first woman-owned radio station, she addresses critical issues such as livelihood, gender, governance, and education, aiming to inspire hope and resilience in communities.
Culinary Expert, Founder – Diary of a Northern Cook
Rajaatu Muhammed Ibrahim, popularly known as Chef Rajah, is the culinary genius behind the « Diary of a northern cook » brand which has amassed an impressive following of over 190,000 on instagram.
Chef Rajah shares her passion for cooking, lifestyle, and culture, providing a glimpse into her world through tantalizing recipes and engaging storytelling.
Amanda Chenai Makombe is a versatile professional excelling in creative design, research, and project management. As the founder of Kumbekumbe Arts Trust, she utilizes various art forms to engage, facilitate, and advocate for community issues, amplifying the voices of young people.
Amanda’s dedication to storytelling and creative expression empowers others and drives positive change in Zimbabwe.
Ada Ujaligwa is a Nigerian-born digital creator, community builder, and lifestyle influencer. Through her Facebook platform where she reaches over 167,000 followers, she shares insights and tips on health, style, fashion, beauty, skincare, and travel.
Her engaging posts and authentic approach make her a trusted voice in the fashion and lifestyle community, impacting lives and fostering a sense of empowerment among her followers.
Angella Summer Namubiru, East Africa’s most-followed TickToker with over 6.2 million followers, engages her audience with her vibrant personality and empowering content. Proud of her dark skin, she uses her platform to advocate for social issues like the dangers of skin bleaching and equal rights for women and children.
Marriage Coach, Founder – Secret Place Wife Community
Bisi Ola Soetan is on a mission to help couples achieve beautiful marriages, God’s way. With expertise in pre-marital and marital counseling, she shares invaluable insights and practical tips for building healthy relationships via her Instagram platform where she reaches over 165,000 followers.
MD- Zetile Oil and Gas, Founder – 360 Woman Africa
Yvonne Ofodile, MD of Zetile Oil and Gas and Founder of 360 Woman Africa, is a leading advocate for women’s entrepreneurship in Nigeria. With over a decade of experience in oil and gas, she empowers women through her digital content and transformational coaching programs.
Yvonne’s impact extends beyond business as she mentors aspiring women entrepreneurs through platforms like the Academy of Women Entrepreneurs.
CEO – ECAir, President of The African Education Foundation (AEF)
Fatima Beyina-Moussa is a trailblazing leader in African aviation, renowned as the CEO of ECAir, the national airline of the Republic of Congo.
Additionally, Beyina-Moussa serves as President of the African Education Foundation, demonstrating her commitment to advancing education and socioeconomic development in Africa.
General Manager of the Lagos State Office for Disability Affairs.
Adenike Oyetunde-Lawal is a multifaceted professional, radio host, lawyer, and life coach. As the founder of Amputees United Initiative and The Gratitude Hub, she empowers persons with disabilities and fosters gratitude through her initiatives and digital content.
She currently serves as the General Manager of the Lagos State Office for Disability Affairs.
Lulu Limbikani, co-founder of Cumacatu, champions girls’ and women’s empowerment in Zambia. Through education and training sessions, Cumacatu provides back-to-school support and fosters basic financial literacy and farming skills.
Lulu’s commitment to education and technology integration in the classroom drives her advocacy for lifelong learning and gender empowerment.
Ella Chioma Ezeadilieje, a seasoned storyteller, helps businesses craft compelling narratives to enhance brand engagement. Through her digital content, ebooks, and live training, she empowers brands to connect with their audience on a deeper level, impacting lives and forging stronger connections in the process.
Rebecca Enonchong, a pioneering tech entrepreneur from Cameroon, founded AppsTech, a global enterprise applications provider. Recognized by the World Economic Forum and Forbes, she’s celebrated for her advocacy in promoting technology in Africa.
Enonchong’s Twitter presence as @Africatechie has garnered over 200,000 followers, establishing her as a leading voice in African tech circles.
Founder – 100 Women @Davos, Global Women’s Leadership Expert
Dr. Anino Emuwa, an internationally recognized management consultant, leads the innovative Avandis Consulting, shaping entrepreneurial ecosystems at the nexus of innovation, finance, and human capital development.
A fervent advocate for gender balance, she spearheads global initiatives like Women@Davos and the African Women CEOs Network.
Ivy Wanjiru Mugo, known as ‘Just Ivy Africa,’ is an acclaimed Digital Creator and Financial Literacy Champion. With her expertise as an Award-Winning Marketer, Ivy empowers individuals through her captivating content and investment insights.
Through ‘The Movers Society,’ she cultivates a vibrant community dedicated to financial enlightenment, personal growth, and enjoyment.
Folake Kehinde, popularly known as Folake Aya Akanni, is a serial entrepreneur and business coach, specializing in marketing and sponsored ads. Through her digital content and innovative training programs, she empowers business owners with the skills and tools to elevate their visibility and drive sales.
Her unique ability to break down complex business concepts into actionable ideas makes her platform stand out.
Eunice Kisiwaa Gyan is a multifaceted young professional, blending her diverse experiences in Human Resources, Diplomacy, compliance, and Media Relations with a strong social media presence, reaching audiences passionate about professional development and cultural enrichment. Notably, she holds a Masters degree in International Affairs and Diplomacy from the University of Ghana and a degree in Political Science from Kwame Nkrumah University of Science and Technology (KNUST).
Chioma Ifeanyi-Eze, a Chartered Accountant and entrepreneur, is dedicated to fostering sustainable growth in African SMEs. With over 11 years of experience in finance and business consulting, she founded AccountingHub in 2015 to provide virtual and retail tech-accounting services tailored to SMEs’ needs.
Through her digital content and training programs, she has supported hundreds of thousands of entrepreneurs in Nigeria, reaching over 160,000 followers via Facebook.
Chief Executive Officer, Strategic Communications Africa Limited
Esther A.N. Cobbah is the CEO and Lead Communication Strategist of Stratcomm Africa Ltd., a top-tier marketing communication agency she founded. With over 35 years of experience in both local and international communications, Esther excels in developing comprehensive strategies utilizing diverse media channels.
Her pioneering work in establishing communication departments for organizations like GNPC and Chevron has left an indelible mark on Ghana’s corporate landscape.
Social Reformer, Leadership Coach, CEO – Meadow Hall Group
Dr. Kehinde Nwani, CEO of Meadow Hall Group and astute educationist, is driven by her passion for leadership excellence.
With over 30 years of experience in building sustainable businesses, she empowers individuals and organizations with proven strategies to build a leadership pipeline for organizational continuity through her digital content and transformational programs.
Associate Director of Africa at the World Economic ForumAbir Ibrahim, a Sudanese-American development practitioner, serves as the Associate Director of Africa at the World Economic Forum in Geneva, Switzerland. With a background in public health and psychology, she has spearheaded impactful initiatives in social and economic development, gender mainstreaming, and global health.
Abir’s mission-driven approach has led to significant contributions, from heading the Private Sector portfolio at UNICEF in Sudan to founding Inua Naturals Inc., empowering marginalized women farmers and artisans.
Toyosi Etim-Effiong, a distinguished media entrepreneur, spearheads That Good Media, promoting authentic African narratives globally. Recognized as one of Nigeria’s inspiring women by Leading Ladies Africa, she empowers aspiring media professionals through workshops, demonstrating her commitment to the growth of Nigeria’s creative sector.
Through her Instagram platform, she reaches over 200,000 followers, sharing inspiring faith-based narratives.
Elizabeth Wanjiru Wathuti, a Kenyan environmentalist and climate activist, founded the Green Generation Initiative to nurture young people’s love for nature and environmental consciousness. Through her initiative, she has planted 30,000 tree seedlings in Kenya, contributing significantly to environmental sustainability and raising awareness about climate change through her digital campaigns.
Madame Joyce, a charismatic media influencer and podcast host of Nigerian descent, captivates audiences with her wit and humor. Co-hosting the podcast “Cocktails and Takeaways” on Apple and Spotify, she delves into human stories while sharing her love for cocktails.
With engaging content on Instagram, Tiktok and YouTube, where she has a combined following of over half a million, she entertains and inspires her followers.
Danièle Sassou Nguesso, Founder of the SOUNGA Foundation, champions education and gender equality through initiatives like Le Petit Samaritain. Her impactful work resonates across Africa, earning her prestigious awards for fostering inclusivity and empowerment.
Media & Social Entrepreneur, Host – Women’s World Show
Clara Chizoba Kronborg is an international media & social entrepreneur, talk show host and creative director. As the host of Women’s World Show and a passionate advocate for diversity and inclusion, Clara has long championed the power of storytelling across various media platforms.
From captivating talk show episodes to visionary content creation and aspiring film productions, her commitment to sparking inspiration and fostering societal change shines through.
Clara Chizoba Kronborg is set to make history with a Guinness World Record attempt for the Longest Interviewing Marathon. The attempt will hold between March 8 and 10 2024, in Marbella, Spain.
Omolabake Matthew, a Social Entrepreneur and Tech Opportunities Advocate, is the founder of Working Mums Diary, and co-founder of Nutrition4kidsng and MumsNTech. She has cultivated a supportive space where mothers can connect, share experiences, and seek guidance on their journey through parenthood.
Through her digital content and innovative programs, she empowers moms to upskill and advance their careers.
Ineza Umuhoza Grace is an eco-feminist and climate activist. As the CEO of The Green Protector and co-founder of the Loss and Damage Youth Coalition, Ineza spearheads transformative efforts to combat climate crisis effects and empower vulnerable communities.
Through advocacy, education, and storytelling, she amplifies youth voices and demands justice for those affected by climate-related loss and damage.
Toyin Onigbanjo is an award-winning child nutrition advocate and founder of August Secrets, a pioneering child nutrition company in Nigeria. Through her innovative cereals, best selling recipe book, and digital content, she aims to combat malnutrition and promote healthy eating habits among African children.
Toyin’s dedication to improving child nutrition has earned her recognition, including the prestigious Graca Machel Gender Lens Award.
Jessica Ufuoma, a Nigerian travel creator and influencer, shares her adventures with her dedicated community of over 200K followers. Through compelling content, she not only inspires others to explore the world. Passionate about travel representation, she aims to empower more people, especially women of color, to embark on their own journeys.
Iyore, a prominent Nigerian-born fashion influencer, captivates audiences with her impeccable sense of style and beauty. Through her vibrant and trend-setting content, she inspires her followers to embrace their individuality and express themselves confidently through fashion.
Rhodaline Nana Animah, Founder and Leader of African YouTubers Hub, is a visionary empowering content creators across Africa. Committed to nurturing creativity and fostering community, she offers vital resources, mentorship, and collaborative opportunities to YouTubers at every stage of their journey.
Vanessa Nakate, a climate justice activist from Uganda, gained prominence in 2018 for raising awareness about the alarming rise in temperatures in her country. Her tireless activism and advocacy, and impactful digital content aim to combat climate change and promote environmental justice on a global scale.
Itiayo Ogunsanwo is a talented photographer renowned for her expertise in concert, event, and portrait photography. As the Head Photographer at BOJ Studios, she leads a team of creatives in producing captivating imagery that tells compelling stories.
Through her Instagram platform, she regularly shares content creation tips to the delight of over 129,000 enthusiasts who currently follow her.
Pelumi Nubi, is a travel content creator, and first Black woman to embark on a solo trip from London to Lagos. On Saturday, January 30th 2024, she embarked on a 2-month solo trip from London to Lagos. Starting from England, Ms Nubi will traverse 17 countries in two months and explore every city and country.
If successful, Ms Nubi will set a record and become the first black woman to drive from London to Lagos, but she said ‘the journey is not about breaking records.’
According to her, it is about showing the world that ‘impossible’ is just a word, especially when someone has enough grit and determination.
Dr. Joy Isa, a seasoned educator and counselor, is dedicated to shaping the future of education in Africa. With extensive experience in international schools and educational leadership roles, she founded the Isa School of Education (ISED) to empower educational leaders across the continent.
As a sought-after facilitator and mentor, Dr. Isa also drives change through her counseling programs and digital content.
Kate Kallot, CEO and Founder of Amini, is pioneering innovative solutions to address the critical issue of data scarcity in Africa. Through her Nairobi-based startup, she harnesses satellite imaging and AI technology to collect and analyze environmental data at a granular level.
Her groundbreaking approach coupled with impactful storytelling empowers communities with actionable insights to tackle pressing environmental challenges, driving positive change for a sustainable future.
Zim Flores, born in Minnesota to Nigerian immigrants, is a serial entrepreneur known for founding the travel company – Travel Noire, which has been acquired by Blavity. As the author of “Dare to Bloom,” she inspires new beginnings. Zim hosts “The Bloom Podcast” and offers faith-based advice through her Instagram platform where she has amassed a following of over 73,000.
Innocencia Ndembara, a software engineer and Director of Women in Tech Malawi, is dedicated to empowering women in technology by providing platforms for skill development and job opportunities.
Through collaborative networks and impactful storytelling, she advocates for equal recognition and opportunities for women in the tech industry
Abcd Africa is a growth marketing and education company that offers world-class online education programs, coaching, and agency services to growth-focused coaches and experts.
We are on a mission to make the voice of the wise be heard.
When we talk of martyrs to many the first thing that comes to mind is the Christians who died for their belief in Jesus Christ and Christianity, and closer to Africa, the martyrs of Uganda, to which most catholic and Anglican churches and establishments derives their names to signify the importance of the actions of the martyrs such as St Kizzito, Charles Lwangwa , St Luke, St Denis among others.
But who is a martyr? To put it simply a martyr is somebody who suffers persecution and death for advocating, renouncing, refusing to comply, obey, and follow what they really believed in or a moral particular cause. Further explanation states that it is a person who suffers very much or is killed because of their religious or political or a believable just cause. These should not be confused with rebellion although to a smaller extent it may link.
…. Martyrdom can be described also as a politically and spiritually explosive performance, done or that happens to achieve a justifiable end.
The questions I would like to ask and try to answer is, do martyrs really matter, are they worthy really remembering, are they worthy to be put in the annuls of history. ? And by extension to the above questions do our own martyr’s closer home Malawi matter worth spending time and thinking about.
I believe they matter. Take for example our own martyrs of Malawi, as 3rd March was declared a public holiday to remember them. In fact, one would wonder whether martyrs matter anymore and whether the day 3rd March is relevant after this long time?, since what the martyrs died for was their own choice, however going deep into the matter one would have a different opinion and surmise that the event should be used to address many more serious national issues and celebrated as a national event.
It should be noted from the outset that John Chilembwe and his uprising of 1915 is considered as the first Independence Martyr.
The Chilembwe uprising was a rebellion against British colonial rule in Nyasaland (modern-day Malawi) in January 1915. It was led by John Chilembwe, who was educated in America and had seen black American way of life and their struggles. The uprising was based around his church in the village of Mbombwe in Chilazulo. It was centred on the black middle class and encouraged by grievances against the colonial system, including forced labour commonly known as Thangata, discrimination and the new demands on the indigenous population caused by the outbreak of World War I. It is recorded that 40 people were executed by the Police and many more arrested in the revolt aftermath.
Although the rebellion did not itself achieve lasting success, it is commonly cited as a watershed moment in Nyasaland history. The rebellion had lasting effects on the British system of administration in Nyasaland and some reform was enacted in its aftermath.
Today, the uprising of 1915 is celebrated annually and Chilembwe himself is considered a national hero and martyr. The climax of this discussion being the martyrs of 1959 mostly those who died in Nkhatabay.
Over the years Malawians have had different views on this day and issue (martyrs day) some positive for the day others negative, for example on 3rd March 2016 during an interview – Veteran Politician Robson Chirwa decried Martyrs Day’s loss of its significance.
“Well Kamuzu was a disciplinarian and he knew what this day meant to the Malawi nation … “My plea is that this day should be declared as a National Day of Mourning as it was the case … Very few can do that in the current political world.’ To this end he was simply signifying that martyrs do matter in society and Malawi in particular.
However, others have the view that it is a waste of time to remember the fallen martyrs, as they believe things could have changed anyway. (This category perhaps lacks details and a background why they the martyrs should matter ;).
Malawians had been living under oppression under laws that were against their favor as owners of the land and they started mobilizing themselves to seek justice and freedom.
In retaliation, the British Government arrested Malawians “Operation Sunrise was the name given to a police and military action conducted by the authorities in the Central African country of Nyasaland (now known as Malawi) on March 3, 1959 to detain and intern 350 individuals who were considered a potential threat to law and order. Thirty-three innocent people lost their lives on this particular day and by 4th March several Malawians were arrested and detained.
The British government was calling for tolerance to which the people tolerated all they could but after some time they said enough was enough. Personally, I find it unreasonable for the British to expect from Malawians tolerance and win win situations what they were entirely unwilling to give.
To further signify the importance of the martyrs, in 2015 third March, martyrs’ day was commemorated in Nkhata Bay district and the day was a Tuesday. To show that Malawi still considers the martyrs with a strong conviction and that they matter a call for, the then Malawi’s colonial master, Britain was asked to compensate 33 families whose relatives died after being massacred by colonial forces in Nkhata Bay district.
At a somber ceremony which was graced by Minister of Finance, Economic Planning and Development, late Dr. Goodall Gondwe as guest of honor, Nkhata Bay Central parliamentarian Ralph Mhone then asked Britain to compensate the families of the deceased since it is their authorities then who commissioned the massacre of the 33 people.
“The 33 deceased families here are mourning year in and year out. As you all might be aware, in the process of killing their relatives, they created a lot of challenges to families because some of those killed were bread winners.
“It should also be borne in mind that apart from creating economic and social challenges to such families, the mere fact that they were innocently killed warrants compensation from those responsible,” said Mhone.
The parliamentarian further asked Malawi Government to take the MV Mpasa ship to Nkhata Bay district. The ship was used by colonial masters to detain the Nyasaland African Congress (NAC) supporters on 3 March 1959, a situation which prompted a mob of Malawians to angrily call for their release and resultant massacre.
Efforts have been made or rather are still being made to make sure the martyrs are compensated for they died for a cause.
To this end Malawians of goodwill must feel that actions through death were necessary to their cause, furthering the truth and their sacrifices cannot be simply a private matter between themselves and their deity, but to the nation as a whole.
It is a fact that with the passing of time things do change and facts become twisted to suit a particular sect of society for their selfish ends but the fact still remains that the issues happened that qualify the victims to be martyrs and to be in the pages of the history of Malawi as issues that matter.
To know that they really matter perhaps we need to see it in the rights and privileges we enjoy today as a people of Malawi their self-belief shaped the course of the nation.
It should not be looked upon as an occasion for complacent acquiescence that sits uneasily with martyrdom. Further to that, we need to see in the action of the martyrs an opening up of the possibility of a deeper understanding of what peace and freedoms are, that peace and freedom are not inevitable, but often come at a cost and heavy price as paid by the 1915 uprising of Chilazulo and the 1959 massacre in Nkhatabay.
This is not only a cost paid first and foremost by a God who loves us so much that he died for us on the cross, but is also paid by his followers who are prepared to follow in his steps, to offer up their lives to uphold the peace and freedom of their own consciences and so to protect the peace and freedom of ours. It is no dispute that their selfless act in making sure their voices were heard makes us proud and proud we must be.
In times of concord and merry making, at least some of us risk forgetting the martyrs in the sense that really matters, but in so doing we risk forgetting the cost that has been paid for our peace and freedom and so risk devaluing the peace and freedom we enjoy. We thank God for the grace of all martyrs, and let us celebrate our peace and our freedom with something of the gratitude that they deserve.
Further to that, to show that we care and that they matter, every year prayers remembering the martyrs are held and the day is a public holiday. Memorial pillars have been erected to signify the importance of the martyrs.
Did they die in vain, did they shed blood in vain? are we wasting out our energies in remembering them? Should we remember them as foot soldiers? In my view they did not die in vain. It is therefore important that they be remembered every year and perhaps a video documentary be done for future generations to understand what it was.
In conclusion, it is my considered view that the martyrs really matter as the events of March 1959 triggered the wheels of change. This should be noted that it was the last straw that broke the camel’s back as from that moment the colonial masters knew that there was no turning back discussions started of giving freedom to the owners of the land. This then means the martyrs did not die in vain.
The question is would we have done the same if we were in their shoes? Would we have continued to chicken out, or we would have sacrificed our lives for future generations?
By Stevie Kauka
The author is a Fellow of IPMM who writes on various topics in his own personal capacity