Lilongwe, Malawi – Moyenda Mutharika Knapp, daughter of former Malawi President Peter Mutharika, has been shortlisted for recognition among the 100 Top Black American Lawyers in the USA by the National Black Lawyers Association.
The association highlights Mutharika Knapp’s distinguished legal career, noting her in-house law firm experience in handling employment law, commercial litigation, and long-term disability matters.
Moyenda is admitted to the Illinois State Bar and has built a reputation in the U.S. legal profession through her extensive litigation and advocacy work. In addition to practicing law, she has served as an adjunct professor at Northwestern University Pritzker School of Law since 2005, teaching trial advocacy and civil discovery.
Her dual role as a practicing attorney and legal educator has positioned her as a mentor and role model within the legal community.
Recognition in a Competitive Field
With over 1.3 million active lawyers in the United States, according to the American Bar Association, being shortlisted among the top 100 is a significant milestone that underscores her exceptional contribution to the legal profession.
Back home, legal experts have applauded the recognition. Professor Ngeyi Kanyongolo, a respected legal scholar in Malawi, described the achievement as a testament to excellence and perseverance.
“This recognition speaks to a high level of excellence and is an inspiration to many lawyers, especially female lawyers in Malawi,” said Kanyongolo.
Moyenda Mutharika Knapp’s recognition not only celebrates her personal success but also places Malawi on the global legal stage. Her story serves as an inspiration to young legal professionals in Malawi and across Africa who aspire to achieve international recognition.
We are continuing our new series, Media Day, where we spotlight individual medical institutions and infectious disease (ID) programs. Today, we spotlight UNC’s Institute for Global Health and Infectious Diseases (IGHID).
There are a number of concerning issues and barriers associated with PrEP access including insurance limitations, stigma, logistics, and awareness. It is this last issue, awareness, and limited educational opportunities that can make a significant difference in people accessing this form of HIV prevention, according to Sarah Rutstein, MD, PhD, assistant professor of medicine at School of Medicine at UNC in the Division of Infectious Diseases.
In her work overseas and in the US, Rutstein says one of the major differences is which sexes have been vulnerable to HIV in the US compared to Africa and specifically Malawi, a resource-depleted country.
“In the southeastern United States, we often think about men who have sex with men, and increasingly, now heterosexual women of African American descent. And historically in Malawi, the prime population that has been vulnerable to HIV has been adolescent girls and young women…To really make it clear, this is not about trying to single out one population based on whatever stereotypes or whatever sort of assumptions you’re making about who they’re having sex with.”
In Rutstein’s work, one of the biggest things she and colleagues have seen is that men do not engage in health care the way that women did.
“They’re [men] not coming in for antenatal care or family planning, or a lot of the other ways that we engage young women in Malawi in the health care system, and therefore, get an opportunity to educate them about PrEP and HIV prevention,” Rutstein said. “Men just don’t have that same access to health services. And we see the exact same thing here in the United States, where we’re looking at, how do we reach people who aren’t otherwise engaging in health services? And it turns out, [sexually transmitted infections] STI clinics, if you have an STI, you’re going to go in and you’re going to try and get it treated.”
In Malawi they integrated PrEP into one the largest urban STI clinics there. Taking that model, and applying it domestically, there were calls for applications from the National Institutes of Health to think about integrating PrEP into STI services in the US. And this seemed like an expansion of the work they had been doing in Malawi, according to Rutstein.
“I think it speaks to the unique opportunity to really take a lot of the lessons that we learned in low resource income settings like Malawi and apply them to other similarly very low resource settings here in the United States—where rural North Carolina certainly fits that bill,” Rutstein said.
While she notes that awareness and education are crucial, structural barriers are really the biggest access issues in the US today.
“It is this cost of the medication, the access to the blood tests that are needed to appropriately start,” Rustein said. “So, I think comfort with providers and actually prescribing and knowing, once I prescribe it, how are they actually going to get this medication? and how do I safely counsel them about the safety of staying on or safely coming off when they perceive themselves to no longer need it?”
In the next episode, Jonathan Parr, MD, MPH, details his work on a genomic sequencing project and how it is being used to monitor drug-resistant malaria.
The global response to HIV, which has spanned several decades,1,2 is currently at an inflection point. By 2023, the number of individuals receiving life-saving antiretroviral therapy had reached nearly 31 million, while the number of those living with HIV who were not receiving such therapy stood at 9.3 million. This public health success has led to a significant reduction in the number of AIDS-related deaths, which have now reached their lowest level since the peak in 2004.1
In the Democratic Republic of Congo, the epidemic is considered generalized (with a low prevalence of 1.2%, a seroprevalence rate of 1.6% in women aged 15 to 49 years and 0.6% in men of the same age), with epidemic foci in mining communities (Haut-Katanga and Lualaba) and urban centers of Kinshasa.3
The international community’s commitment to the Sustainable Development Goals (SDGs) has led to significant progress in the fight against HIV, with the eradication of HIV as a public health threat being considered a realistic possibility by 2030. However, the accession to power of the new US administration has led to a setback in these efforts, jeopardising the progression of HIV as a public health threat.4,5 However, the continued provision of “life-saving humanitarian assistance” has been facilitated by UNAIDS, which has obtained an exemption, thus ensuring the continuation or resumption of essential medicines and medical services, including HIV treatment, as well as the necessary supplies for this assistance. Furthermore, UNAIDS has committed to the continuation of its efforts in favour of other essential components of the PEPFAR (Emergency Programme of Health and HIV Prevention Services, Care and Support for Orphans and Vulnerable Children) initiatives.4
In this context of uncertainty, it becomes imperative to explore ways to improve the psychosocial and economic support provided to these Children people in a country facing aggression from armed groups. HIV/AIDS is now considered a chronic disease, causing not only physical health complications.6
This situation also affects Children people living with HIV, and is accompanied by a large number of children entering adolescence and adulthood with a chronic infectious disease, thanks in particular to psychosocial and economic support services.7
However, existing research reveals a lack of psychosocial and economic support for children and young people living with HIV (CPLHIV). Existing research shows that young people living with HIV do not receive sufficient psychosocial and economic support7–11. A review demonstrated that treatment adherence, disclosure of HIV status, gender-related issues and lack of support networks are problems faced by CPLHIV across the world.
In the DRC, particularly in Lubumbashi, health and community professionals play a key role in providing holistic care and treatment for people living with HIV, especially young people. As front-line workers, they have a comprehensive understanding of the challenges faced by children living with HIV and how these challenges are perceived and experienced, including those not expressed by the children themselves. This perception of the psychosocial and economic challenges faced by children living with HIV can therefore inform the design of viable policies and programmes.12–17 Our study also includes community members, such as adolescent and adult peer educators, providing a broader view of the situation.18
This study therefore aims to determine the challenges requiring psychosocial and economic support faced by Children living with HIV, to describe the interventions in place and to explore the experience of professionals providing psychosocial support to Children people living with HIV in Lubumbashi, in the current context of uncertainty.
Methods
Study Framework
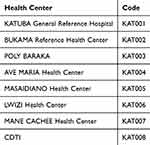
Katuba health zone (Figure 1),19 in the city of Lubumbashi, capital of the Haut-Katanga province in the Democratic Republic of Congo. It involved eight structures in this zone: the KATUBA General Reference Hospital, the BUKAMA Reference Health Center, the POLY BARAKA, the CDTI Health Center, the AVE MARIA Health Center, the MASAIDIANO Health Center, the LWIZI Health Center and the MANE CACHEE Health Center (Table 1). All these health care establishments (ESS) were targeted because they have an HIV/AIDS care service.
Table 1 List of ESS
Figure 1 Health map of the city of Lubumbashi, DRC, subdivided into health zone and Katuba health zone surrounded by a red frame.
Study Design
The present study adopted a descriptive case study approach,20 employing a phenomenological qualitative method, in order to ascertain the psychosocial and economic support care provided to persons living with HIV (PLHIV).21,22 In order to achieve the objectives of the study, the views of providers and community workers (case managers and peer educators) were canvassed. The research took place over an eight-month period, from June 1, 2024 to February 8, 2025, with data collection between July 1 and August 1, 2024.
Sampling
The study covered all staff working in the field of CPLHIV care in health facilities in the Katuba Health Zone. The study population was organized into three hierarchical levels: the focal points of each health facility, then the peer educators and the case managers. In order to ensure optimal representativeness of the study population, targeted (or purposive) sampling was methodically applied for the recruitment of participants. They have been grouped according to the department in which they work: Appui Psychosocial (APS) and Orphelin et Enfants Vulnerables (OVC)., in order to ensure the homogeneity of the sample; without distinction of sex (mixture of men and women).
Inclusion Criteria
We included in the study only those who had at least six months of direct experience with CPLHIV (Table 2). All participants were over 18 years old. According to the DRC Constitution, as amended, a child is any person under the age of 18.23
Table 2 Study Participants
Recruitment of Study Participants
Before the start of each in-depth, face-to-face, semi-structured interview with providers and peer educators, or each non-directive focus group session with case managers, participants were contacted and given an information sheet and an informed consent form. Due to the locations of the participants and the configuration of their workplaces, semi-structured interviews were conducted with all participants, while focus groups were conducted with case managers only. Participants who consented to participate in the study were instructed to not limit themselves to the list of questions and to iterate until information saturation was reached.
The in-depth, semi-structured interviews lasted between 45 and 60 minutes, while the focus groups lasted between 75 and 90 minutes. All interviews were conducted in French, although the participants spoke Swahili. We moderated the sessions and took notes. Our mission was to obtain consent for participation in the study, explain the theme and how the focus groups would be conducted, initiate and encourage discussion, and ensure that participants’ comments were not misinterpreted.
Instruments
The tools used were the interview guide, the Focus Group Guide in French and the Android phone recorder application for recording sounds on themes such as: Challenges that require psychosocial and economic support faced by Children people living with HIV/AIDS, psychosocial and economic interventions, the experience of community caregivers providing psychosocial support to Children people living with HIV/AIDS, psychosocial and economic support and collaboration within the team. These interview guides were developed by reviewing existing literature12,13 and the socio-ecological model14,15 which aims to explore psychosocial and economic support systems among CPLHIV and recognizes that health experiences and outcomes are often influenced by factors intrinsic and extrinsic to the individual.16–18
Data Analysis
The audio recordings were listened to several times before being faithfully transcribed into Microsoft Word and translated (three authors) into French for the Swahili interventions. Before analyzing the data in ATLAS.ti (version 12), the transcripts were imported into the software for content analysis to identify emerging themes associated with the APSC in Lubumbashi.
Reliability
To ensure scientific rigor, we employed criteria of credibility, dependability, transferability, and confirmability19. The audio files were audited several times before being carefully transcribed into Microsoft Word and translated into French by three authors for the Swahili interventions. The supervisory team received the audio recordings, transcriptions, and coding, as well as the themes, to conduct a cross-analysis to ensure the credibility of the results. The lead author (CKD) reviewed the results with other members of the research team (MMM and LNM) as well as his supervisor (CKM). This was made possible through the triangular analysis conducted by the first and fourth authors (CKD and BKP).
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki (1964). Participants gave written informed consent prior to taking part, including consent for the publication of anonymised responses and direct quotes. Authorisation for the research was provided by the faculty. This was for reasons of confidentiality and anonymity. Appropriate data management was ensured in three stages: First, recordings, transcripts and field notes were deleted from the original devices. Second, they were saved in password-protected files on a computer and external hard drive. Finally, they were anonymised. The study obtained research certificate No. 0050/2024 from the Faculty of Medicine at the University of Lubumbashi.
Results
Participant Characteristics
Table 3 presents the sociodemographic characteristics of the respondents. The largest groups were full-time nurses, followed by case managers (28.57%) with an average experience of 15.5 ± 11.43 years (4–34) years. The respondents included were women (57%) and 43% men, with an average age of 44.21 ± 9.40 years.
Table 3 Sociodemographic Characteristics of Respondents
Themes Emergent
Data from eight (8) interviews and one (1) focus group were summarized into three (3) themes which emerged as: Challenges that require psychosocial and economic support faced by Children People Living with HIV/AIDS (i), Psychosocial and Economic Interventions among CPLHIV (ii) and Experience of Community Caregivers Providing Psychosocial Support to CPLHIV (iii). These themes are developed in the following lines (Table 4):
Table 4 Overview of the Main Themes and Their Sub-Themes Relating to Challenges and Interventions in Psychosocial and Economic Support for Children People Living with HIV/AIDS Among Health and Community Workers in the Katuba Health Zone in Lubumbashi, DRC
Theme 1: Challenges That Require Psychosocial and Economic Support Faced by Children People Living with HIV/AIDS
Situation of Children People Living with HIV
Participants shared their experiences of the current challenges faced by Children people living with HIV, which included the burden of treatment and daily adherence to treatment, stigma, and discrimination. Participants also stated that some Children people, in the absence of visible symptoms, struggle to recognize the need for their treatment, which compromises their treatment adherence, and Children people living with HIV experience ridicule, isolation, and discriminatory attitudes from those around them, including those in their families and schools. Participants stated:
[…] Their problem is first of all the effect of taking the medication every day and for an indefinite period. They think that they are not useful to society, that they cannot have children, that they cannot work in life and that they cannot get married, so there are a lot of problems like that […] KAT004
[…] The big problem with these children is adherence to treatment. Physically they don’t feel sick. Their appearance says they’re not sick and they themselves say they’re not sick. So it’s difficult for these children to adhere to treatment and the other problem is that they are mostly orphans so they are mistreated and rejected at times. […] KAT002
The testimonies collected from participants highlight other psychosocial and relational challenges, including the impact of HIV on schooling and socio-professional integration, financial difficulties and access to care, increased vulnerability to abuse and violence, lack of information and fear of disclosure. One participant said:
[…] Children people living with HIV/AIDS, regardless of their age, face multiple and complex challenges. Academic problems: The disease can lead to frequent absences, difficulty concentrating, and decreased academic performance. Relationship difficulties: Children people may have difficulty forming friendships and intimate relationships, due to fear of rejection or transmission of the virus. Uncertainty about the future: The future may seem uncertain, which can generate anxiety and depression. Financial difficulties: Families of Children people living with HIV/AIDS may face financial difficulties related to treatment costs, which can limit access to quality care and essential resources. […] KAT006
Prevention and Psychosocial Support Intervention for Children People Living with HIV/AIDS
Prevention and psychosocial support intervention are a priority, declared all participants, for several reasons justifying this priority: Impact on overall health, prevention of transmission, improvement of life expectancy and reduction of inequalities in all health establishments integrating HIV/AIDS care services. According to them, if these Children people are well prepared, mentally, they will protect themselves and protect others, so it is really a priority. A focal point stated:
[…] If it is an absolute priority, because we must disclose HIV status to Children people and this will allow Children people to know themselves and know how to behave, not to have sex in a disorderly manner, because that could contribute to increasing the number of HIV infections. So, it is also an economic priority, because these Children people living with HIV must be educated and we must prepare them for future life […] KAT002
Awareness of the Psychosocial and Economic Problems of Children People Living with HIV
Participants’ testimonies divide psychosocial and economic problems into two categories: those living with HIV who are aware of the problem and those who are not. This varies depending on their age, social environment, and level of information. Others minimize or deny them. Two focal points summarize this sentiment:
[…] Yes, but well! It depends on the age group. A Children person over 10 is more aware than a Children person under 10. Yes, they consider it an important problem, because they want to know if they will need to get married one day and work like everyone else […] KAT003
[…] Indeed, yes, they are aware because we teach them and they are taught for that. Yes, they consider it as a problem, already the effect of taking the treatment every day while other children their age do not take it and the effect that they live mostly in foster families or in orphanages. Yes, they consider it as a major problem […] KAT006
Questions from Children People Living with HIV
All participants stated that all Children people living with HIV/AIDS face psychosocial and economic challenges. One participant said:
[…] Yes, Children people living with HIV regularly ask questions about psychosocial and economic issues. These questions often concern the future: ‘Will I be able to have a normal life?’ Relationships: ‘Will I be able to find love?’ Work: ‘Will I be able to find a job?’ Education: ‘Will I be able to continue my education?’ […] KAT007
Regarding economic concerns alone, participants stated that community members are more familiar with this concept, and they stated that Children people living with HIV/AIDS require economic support. The most urgent need is access to vocational training. Many of our Children people do not have a diploma and struggle to find employment.
Case Manager 3_FG:
[…] The most urgent need is access to vocational training. Many of our Children people do not have a diploma and have difficulty finding a job. […]
Theme 2: Psychosocial and Economic Interventions for Children People Living with HIV/AIDS
Advice and Management of Children People Living with HIV
Participants stated that the management and counseling of Children people living with HIV/AIDS is done in collaboration with psychosocial workers, other providers do it alone to avoid falls and some entrust this task to social workers, who are there for this situation.
[…] We provide individual and group counseling: Mental health professionals provide a safe space for Children people to express their emotions, concerns, and challenges. Peer support groups: Children people can connect with other Children people living with HIV and share their experiences. Socio-educational activities: Workshops are organized to develop Children people’s social, emotional, and career skills […] KAT006
Children people living with HIV also receive several types of psychosocial support:
[…] We offer active listening, personalized advice, group activities (sharing experiences, self-esteem building workshops) and individualized support. These interventions are effective because they allow Children people to feel supported, develop coping strategies and strengthen their resilience […].CASE MANAGER_3_FG_BKM
Assessment of Psychosocial Risk in Children People Living with HIV
Psychosocial risk assessments for Children people living with providers are conducted by psychosocial workers (case managers and peer educators) and other care providers conduct them alone.
[…] We leave this task to the agents of a non-governmental organization (case manager, peer educators), these social agents have assessment protocols and this allows them to see if they can strengthen psychosocial support […] KAT004
[…] We have a framework, questionnaires that help us to talk with them and to get to the bottom of the problem […] KAT003
Economic Risk Assessment Among Children People Living with HIV
The economic risk assessment is carried out by case managers who are psychosocial agents.
[…] This assessment is done by social workers. For example, there are Children people who have financial difficulties in their family and who need to go to school, they go on site to assess the vulnerability of the family, these agents will judge if the Children people can benefit from the transfer cache. […] KAT003
Effectiveness and Efficiency of Current Psychosocial and Economic Support Assessment and Intervention Services
Current services provided to Children people living with HIV appear efficient and effective for most participants and ineffective for some.
[…] These interventions are effective because they allow Children people to feel supported, develop coping strategies and strengthen their resilience […]. ALL CASE MANAGERS_FG_BKM
[…] It’s not really effective, because the budget we had planned beforehand is not the one we are using today, it’s not working as it should because there are patients who have not received anything until today and we are still waiting, however, the psychosocial support seems to be working […] KAT006
Theme 3: Experience of Community Caregivers Providing Psychosocial Support to Children People Living with HIV
Constraints in Psychosocial and Economic Support Services
Regarding constraints from a psychosocial and economic perspective, the participants’ interview accounts reveal two sides: those who encounter them and those who do not. Among those service providers who encounter obstacles.
[…] Yes, there are constraints, the number of providers is not sufficient, so coverage on the ground seems a little difficult and also the financial subsidy is not sufficient […] KAT003
[…] Here at home, there are no constraints since we started in 2016, in any case, there are no constraints […] KAT008
Recommendations for Improving Psychosocial and Economic Support Services for Children People Living with HIV
All participants made recommendations and challenges to overcome to contribute to better psycho-social and economic support for Children people living with HIV. The strengthening of human and material resources appears first as a first recommendation with the following challenges: the shortage of care providers, the increased need for community workers (case managers and peer educators) and strengthening the training of health professionals. One participant said:
[…] Increase the number of healthcare providers (doctors, nurses, case managers and peer educators) because they are insufficient. For good psychological support, we need a lot of peer educators and a lot of case managers. We also need to increase a lot of efforts because this will allow for good monitoring of Children people living with HIV. For economic support, we only need to increase the budget and then we can improve a lot of things […] KAT004
The second recommendation from the participants concerns increased funding and economic support for JVHIV, better partner funding to ensure business continuity and financial involvement from the government. One participant said:
[…] We must continue to support them. There is also the bad faith of our leaders because the country does not lack the means if we only have to wait for the partners to act; it will not be enough so we ask that the government can help us with funding so that all Children people living with HIV can be cared for, because if the partner left you can imagine what would happen next? […].KAT002
The third recommendation made by the participants was prevention and awareness activities with several challenges. One participant said:
[…] Strengthening prevention: By focusing on primary and secondary prevention, including strengthening sex education and facilitating access to condoms. Combating stigma: By organizing awareness campaigns and involving communities […]. KAT001
The fourth and final recommendation from the interviews was to improve Access to Care and Psychosocial Support, with challenges such as geographical and financial access to care and increased support for families of Children people living with HIV.
[…] Improving access to care: By facilitating geographical and financial access to care, and by strengthening the quality of services offered. Supporting families: By providing psychosocial support to families and involving them in the care of their children. By working together, we can improve the quality of life of Children people living with HIV and empower them to achieve their goals. […] KAT001
Discussion
The present study explores the psychosocial and economic support for CPLHIV as perceived by health workers and community workers in the Katuba health zone. The study identifies the main findings as follows: It is evident that children encounter a multitude of distinctive challenges that exert a detrimental influence on their physical, mental, emotional and social health. The early identification and management of psychosocial and economic issues appear to be pivotal in enhancing their overall well-being. While the efficacy of current psychosocial and economic interventions is acknowledged, there is a consensus that their effectiveness could be enhanced. The recommendations made by the service providers surveyed underscore the necessity to fortify the support system in its entirety, encompassing both human resources and organisational arrangements.
CPLHIV face a multitude of specific challenges that influence their physical, mental, emotional and social health. These challenges vary depending on the social environment, population, culture and the broader socio-economic and political context.24 As reported by the participants in our study who reported as challenges the burden of treatment, daily therapeutic adherence, stigma and discrimination, including social and academic rejection. Other participants also mentioned various situations that CPLHIV may face, such as the effect of HIV on education and professional integration, economic problems and access to care, increased susceptibility to abuse and violence, information deficit and fear of exposure24–28. The results of this study are consistent with those of several research studies that have highlighted issues such as personal stigma, isolation and adjustment problems. These issues can significantly impact people’s ability to adhere to antiretroviral therapy, their independence, and their ability to establish and maintain healthy social relationships24–27. For example, it has been reported that some people, in the absence of visible symptoms, struggle to recognize the need for treatment, which compromises their treatment adherence. Some CPLHIV avoid social interactions and do not seek the necessary social support, believing that they do not deserve respect or attention. This dynamic can lead to a state of hopelessness and a constant fear of rejection, without the social support they desperately need.24–27
The findings of this study, supported by,29 highlight the critical importance of comprehensive psychosocial and economic interventions to provide CPLHIV with more tailored coping strategies and support systems in light of the challenges identified. Psychosocial support is an essential component of holistic care for these CPLHIV. Indeed, it has been shown that this support enables Children people to cope with the emotional, social and economic challenges related to their diagnosis, to improve their self-esteem and to develop life skills.
However, in low-resource settings, health systems often face challenges in supporting populations in managing these multifaceted challenges. These difficulties are exacerbated by various factors compounded by the suspension of PEPFAR assistance, including limited government attention, armed conflict in the case of the DRC, population displacement, and political instability.30,31
Regarding psychosocial and economic interventions for CPLHIV, stakeholders highlighted that support and guidance, as well as assessment of psychosocial and economic risks for these individuals, are primarily carried out in collaboration with community members. Psychosocial and economic interventions can be effectively deployed to improve adherence to antiretroviral therapy among HIV-positive adolescents and Children adults in resource-limited settings,32–34 as demonstrated by several studies, including ours. These findings are consistent with several studies that have demonstrated increased retention and adherence to antiretroviral therapy (ART) among adolescents and Children people following the application of a psychosocial method.9,32,34–42
Early identification and intervention of psychosocial and economic problems are crucial. The data collected reveal a variety of circumstances associated with the challenges encountered in implementing psychosocial and economic support services for people living with HIV. On the one hand, various participants reported problems related to insufficient human and financial resources. On the other hand, others reported not encountering any major obstacles.
Research has shown that initiatives aimed at strengthening support networks, improving the training of health professionals and promoting community actions can have a decisive influence on improving the quality of life of people living with HIV and their caregivers.43–45
Strasser et al46 argue that evidence-based psychosocial and economic support services for CPLHIV are currently underdeveloped and underfunded. They state that this situation needs to be addressed and improved, as some participants attested. The sudden interruption of current development assistance or future reduction of PEPFAR funding may negate efforts made so far towards the elimination of HIV/AIDS as a health problem36. The goal of ending the AIDS pandemic by 2030 is within reach, urgent action is needed from world leaders20, particularly in sub-Saharan Africa, which concentrated more than 90% of the funding and was home to two-thirds of all people living with HIV.37,38
Strength and Limits
The primary strength of this study lies in the diversity of the participants, encompassing various genders, age ranges, and roles, thereby facilitating an in-depth exploration of the realities experienced by CPLHIV. Notwithstanding, this study is not without its limitations. Primarily, the research design, employing a case study approach guided by a phenomenological method, renders the findings inherently bound to the context of the Katuba health zone. It is acknowledged that each health zone possesses its own unique characteristics, which serve to distinguish it from other health zones. Consequently, it is posited that the results of this research may only be applicable to other zones that exhibit similar contexts. Secondly, the study of the challenges faced by young people can only be better understood through the application of socio-ecological approaches, which emphasise the interaction between the different levels (individual, family, community, institutional).47 This study did not achieve this.
Future research endeavours could concentrate on the challenges confronted by CPLVHIV. This could be achieved by investigating the perspectives of family members, young people themselves, community workers and healthcare staff.
Conclusion
This research highlights a series of challenges faced by children living with HIV that have a deleterious influence on their overall well-being. It highlights the need for early identification and management of these challenges, in order to significantly improve the quality of life of the individuals concerned. Although current interventions are considered effective, there is a consensus that their effectiveness could be improved. This could be achieved by strengthening the support system through recommendations from service providers, particularly in terms of human resources and organisation. As part of our recommendations for future interventions or the adjustment of existing interventions, we advocate the strengthening of human and material resources in order to meet the following challenges: the shortage of healthcare providers; the increased needs of community members and their training; increased funding, in particular the financial involvement of the national government; focusing on more prevention and awareness-raising activities; improving access to care and support for the families of children living with HIV. These strategies should be implemented to reduce the psychological and economic distress of children living with HIV. To achieve this, the various stakeholders should be involved with a view to “eliminating HIV/AIDS by 2030”. Further research could be carried out in all the health zones of the city of Lubumbashi, using qualitative or mixed methodologies as part of a socio-ecological approach.
Abbreviation
CPLHIV, Children people living with HIV/AIDS.
Data Sharing Statement
The original contributions to this study are presented in the article, and the transcripts and other supporting material for this manuscript are available from the corresponding authors and publishers.
Disclosure
No competing interests have been declared by the authors.
3. Ministère du Plan et Suivi de la Mise en œuvre de la Révolution de la Modernité-MPSMRM/Congo. Ministère de la Santé Publique-MSP/Congo, ICF International. République Démocratique du Congo Enquête Démographique et de Santé (EDS-RDC) 2013–2014. 2014.
5. Lancet T. American chaos: standing up for health and medicine. Lancet. 2025;405(10477):439. doi:10.1016/S0140-6736(25)00237-5
6. Bravo P, Edwards A, Rollnick S, Elwyn G. Tough decisions faced by people living with HIV: a literature review of psychosocial problems. AIDS Rev. 2010;12(2):76–88.
7. Greifinger R, Dick B. Provision of psychosocial support for young people living with HIV: voices from the field. SAHARA-J J Soc Asp HIVAIDS. 2011;8(1):33–41. doi:10.1080/17290376.2011.9724982
8. Nyongesa MK, Nasambu C, Mapenzi R, et al. Psychosocial and mental health challenges faced by emerging adults living with HIV and support systems aiding their positive coping: a qualitative study from the Kenyan coast. BMC Public Health. 2022;22(1):76. doi:10.1186/s12889-021-12440-x
9. Petersen I, Bhana A, Myeza N, et al. Psychosocial challenges and protective influences for socio-emotional coping of HIV+ adolescents in South Africa: a qualitative investigation. AIDS Care. 2010;22(8):970–978. doi:10.1080/09540121003623693
10. Mutumba M, Bauermeister JA, Musiime V, et al. Psychosocial challenges and strategies for coping with HIV among adolescents in Uganda: a qualitative study. AIDS Patient Care STDs. 2015;29(2):86–94. doi:10.1089/apc.2014.0222
11. Ramaiya MK, Sullivan KA, Donnell KO, et al. A Qualitative Exploration of the Mental Health and Psychosocial Contexts of HIV-Positive Adolescents in Tanzania. PLoS One. 2016;11(11):e0165936. doi:10.1371/journal.pone.0165936
13. Stevens A, Gabbay J. Needs assessment needs assessment. Health Trends. 1991;23(1):20–23.
14. Mulenga DM, Rosen JG, Banda L, et al. “I have to do it in secrecy”: provider Perspectives on HIV Service Delivery and Quality of Care for Key Populations in Zambia. J Assoc Nurses AIDS Care JANAC. 2024;35(1):27–39. doi:10.1097/JNC.0000000000000443
15. Igihozo G, Sichali JM, Medhe S, Wong R. Exploring the Perspectives of Healthcare Providers on Providing HIV Prevention and Treatment Services for Key Populations in Rwanda: a Qualitative Study. World J AIDS. 2022;12(2):120–139. doi:10.4236/wja.2022.122010
16. Yannessa JF, Reece M, Basta TB. HIV Provider Perspectives: the Impact of Stigma on Substance Abusers Living with HIV in a Rural Area of the United States. AIDS Patient Care STDs. 2008;22(8):669–675. doi:10.1089/apc.2007.0151
17. Mutambo C, Hlongwana K. Healthcare Workers’ Perspectives on the Barriers to Providing HIV Services to Children in Sub-Saharan Africa. AIDS Res Treat. 2019;2019:1–10. doi:10.1155/2019/8056382
18. Medley A, Kennedy C, O’Reilly K, Sweat M. Effectiveness of Peer Education Interventions for HIV Prevention in Developing Countries: a Systematic Review and Meta-Analysis. AIDS Educ Prev. 2009;21(3):181–206. doi:10.1521/aeap.2009.21.3.181
19. Chenge M, Van der Vennet J, Porignon D, Luboya N, Kabyla I, Criel B. La carte sanitaire de la ville de Lubumbashi, République Démocratique du Congo Partie I: problématique de la couverture sanitaire en milieu urbain congolais. Glob Health Promot. 2010;17(3):63–74. doi:10.1177/1757975910375173
20. Lucy G. Recherche Sur Les Politiques et Les Systèmes de Santé: Manuel de Méthodologie: Version Abrégée. Alliance pour la recherche sur le politiques et les systèmes de santé. Organisation mondiale de la Santé; 2013.
21. Corbiére M, Larivière N. Méthodes Qualitatives, Quantitatives et Mixtes, 2e Édition: Dans La Recherche En Sciences Humaines, Sociales et de La Santé. 2nd ed ed. Presses de l’Université du Québec. 2020. doi:10.2307/j.ctv1c29qz7
22. Creswell JW, Creswell JD. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. 6th ed ed. Sage Publications, Inc; 2022.
23. Cabinet du Président de la République. Constitution de la République Démocratique du Congo telle que révisée par la Loi n° 11/002 du 20 janvier 2011 portant révision de la Constitution de la République Démocratique du Congo du 18. (Textes coordonnés). 2011. Available from: https://www.leganet.cd/Legislation/JO/2011/JOS.05.02.2011.pdf. Accessed June 9, 2025.
24. Adraro W, Abeshu G, Abamecha F. Physical and psychological impact of HIV/AIDS toward youths in Southwest Ethiopia: a phenomenological study. BMC Public Health. 2024;24(1):2963. doi:10.1186/s12889-024-20478-w
25. Getaye A, Cherie N, Bazie GW, Gebremeskel Aragie T. Proportion of Depression and Its Associated Factors Among Youth HIV/AIDS Clients Attending ART Clinic in Dessie Town Government Health Facilities, Northeast Ethiopia. J Multidiscip Healthc. 2021;14:197–205. doi:10.2147/JMDH.S296849
26. Tamirat KS, Tesema GA, Tessema ZT. Psychosocial Factors Associated with Suicidal Ideation Among HIV/AIDS Patients on Follow-Up at Dessie Referral Hospital, Northeast Ethiopia: a Cross-Sectional Study. HIV/AIDS – Research and Palliative Care. 2021;13:415–423. doi:10.2147/HIV.S299538
27. Duko B, Toma A, Asnake S, Abraham Y. Depression, anxiety and their correlates among patients with HIV in South Ethiopia: an institution-based cross-sectional study. Front Psychiatry. 2019;10:290. doi:10.3389/fpsyt.2019.00290
28. Mutumba M, Musiime V, Lepkwoski JM, et al. Examining the relationship between psychological distress and adherence to anti-retroviral therapy among Ugandan adolescents living with HIV. AIDS Care. 2016;28(7):807–815. doi:10.1080/09540121.2015.1131966
29. Parcesepe A, Tymejczyk O, Remien R, et al. HIV-Related Stigma, Social Support, and Psychological Distress Among Individuals Initiating ART in Ethiopia. AIDS Behav. 2018;22(12):3815–3825. doi:10.1007/s10461-018-2059-8
30. Mirkuzie AH, Ali S, Abate E, Worku A, Misganaw A. Progress towards the 2020 fast track HIV/AIDS reduction targets across ages in Ethiopia as compared to neighboring countries using global burden of diseases 2017 data. BMC Public Health. 2021;21(1):285. doi:10.1186/s12889-021-10269-y
31. Girum T, Wasie A, Worku A. Trend of HIV/AIDS for the last 26 years and predicting achievement of the 90–90-90 HIV prevention targets by 2020 in Ethiopia: a time series analysis. BMC Infect Dis. 2018;18(1):320. doi:10.1186/s12879-018-3214-6
32. Okonji EF, Mukumbang FC, Orth Z, Vickerman-Delport SA, Van Wyk B. Psychosocial support interventions for improved adherence and retention in ART care for young people living with HIV (10–24 years): a scoping review. BMC Public Health. 2020;20(1):1841. doi:10.1186/s12889-020-09717-y
33. Hudelson C, Cluver L. Factors associated with adherence to antiretroviral therapy among adolescents living with HIV/AIDS in low- and middle-income countries: a systematic review. AIDS Care. 2015;27(7):805–816. doi:10.1080/09540121.2015.1011073
34. Bhana A, Mellins CA, Petersen I, et al. The VUKA family program: piloting a family-based psychosocial intervention to promote health and mental health among HIV infected early adolescents in South Africa. AIDS Care. 2014;26(1):1–11. doi:10.1080/09540121.2013.806770
35. Davila JA, Miertschin N, Sansgiry S, Schwarzwald H, Henley C, Giordano TP. Centralization of HIV services in HIV-positive African-American and Hispanic youth improves retention in care. AIDS Care. 2013;25(2):202–206. doi:10.1080/09540121.2012.689811
36. Ruria EC, Masaba R, Kose J, et al. Optimizing linkage to care and initiation and retention on treatment of adolescents with newly diagnosed HIV infection. Aids. 2017;31:S253–S260. doi:10.1097/QAD.0000000000001538
37. Wohl AR, Garland WH, Wu J, et al. A youth-focused case management intervention to engage and retain young gay men of color in HIV care. AIDS Care. 2011;23(8):988–997. doi:10.1080/09540121.2010.542125
38. Willis N, Milanzi A, Mawodzeke M, et al. Effectiveness of community adolescent treatment supporters (CATS) interventions in improving linkage and retention in care, adherence to ART and psychosocial well-being: a randomised trial among adolescents living with HIV in rural Zimbabwe. BMC Public Health. 2019;19(1):117. doi:10.1186/s12889-019-6447-4
39. Graves JC, Elyanu P, Schellack CJ, et al. Impact of a family clinic day intervention on paediatric and adolescent appointment adherence and retention in antiretroviral therapy: a cluster randomized controlled trial in Uganda. PLoS One. 2018;13(3):e0192068. doi:10.1371/journal.pone.0192068
40. Uusküla A, Laisaar KT, Raag M, et al. Effects of Counselling on Adherence to Antiretroviral Treatment Among People with HIV in Estonia: a Randomized Controlled Trial. AIDS Behav. 2018;22(1):224–233. doi:10.1007/s10461-017-1859-6
41. Tominari S, Nakakura T, Yasuo T, et al. Implementation of mental health service has an impact on retention in HIV care: a nested case-control study in a japanese HIV care facility. PLoS One. 2013;8(7):e69603. doi:10.1371/journal.pone.0069603
42. MacKenzie RK, Van Lettow M, Gondwe C, et al. Greater retention in care among adolescents on antiretroviral treatment accessing “Teen Club” an adolescent‐centred differentiated care model compared with standard of care: a nested case–control study at a tertiary referral hospital in Malawi. J Int AIDS Soc. 2017;20(3):e25028. doi:10.1002/jia2.25028
43. Baingana F, Thomas R, Comblain C. HIV/AIDS and mental health. The World Bank, Health Nutr Popul HNP Discuss Pap. 2005;2005;1–65.
45. Pagano L, Caira M, Offidani M, et al. Adherence to international guidelines for the treatment of invasive aspergillosis in acute myeloid leukaemia: feasibility and utility (SEIFEM-2008B study). J Antimicrob Chemother. 2010;65(9):2013–2018. doi:10.1093/jac/dkq240
46. Strasser S, Gibbons S. The development of HIV-related mental health and psychosocial services for children and adolescents in Zambia: the case for learning by doing. Child Youth Serv Rev. 2014;45:150–157. doi:10.1016/j.childyouth.2014.03.032
47. Richard L, Gauvin L, Raine K. Ecological Models Revisited: their Uses and Evolution in Health Promotion Over Two Decades. Annu Rev Public Health. 2011;32(2011):307–326. doi:10.1146/annurev-publhealth-031210-101141
The opinions expressed in all articles published here are those of the specific author(s), and do not necessarily reflect the views of Dove Medical Press Ltd or any of its employees.
Dove Medical Press is part of Taylor & Francis Group, the Academic Publishing Division of Informa PLC Copyright 2025 Informa PLC. All rights reserved. This site is owned and operated by Informa PLC ( “Informa”) whose registered office is 5 Howick Place, London SW1P 1WG. Registered in England and Wales. Number 3099067. UK VAT Group: GB 365 4626 36
American singer, songwriter, and dancer Ciara has officially received citizenship in Benin, becoming one of the growing number of African-American celebrities reconnecting with their ancestral roots through African citizenship.
The 36-year-old artist shared the news on her official Facebook page, revealing that she was granted Beninese nationality on July 26, during this year’s United Nations International Day of Women and Girls of African Descent. Notably, Ciara is the first person in the world to be granted citizenship under Benin’s new initiative to welcome members of the African diaspora.
“July 26, history was made. On this year’s United Nations International Day of Women and Girls of African Descent, I was honored to receive Beninese citizenship, becoming the first person in the world granted nationality under this new initiative! To be welcomed by His Excellency President Patrice Talon, the Office of Benin Tourism, and the beautiful people of Benin is a moment I will never forget,” Ciara wrote.
The singer also paid tribute to Benin’s historic city of Ouidah, one of the busiest slave ports during the transatlantic slave trade, acknowledging the painful past and the importance of reconnecting with her ancestral roots.
Ciara now joins a list of prominent black folk in America who have reclaimed African citizenship, including Tiffany Haddish, Stevie Wonder, Samuel L. Jackson, and Ludacris.
As more members of the Black diaspora trace their lineage to Africa, initiatives like Benin’s are helping to heal historical wounds and celebrate cultural reconnection.
Malcolm Brogdon might be known to NBA fans as a steady, intelligent, and efficient point guard. The 2017 Rookie of the Year, 2023 Sixth Man of the Year, and a consistent performer from the free-throw line and beyond the arc. But the roots of his character stretch far deeper than basketball. His impact off the court is just as powerful. From childhood, Brogdon was raised with a sense of purpose, identity, and service values instilled in him by his remarkable parents, Mitchell Gino Brogdon and Dr. Jann Adams.
Named after Malcolm X, Brogdon has always had a deep understanding of his role in society. His upbringing wasn’t accidental…it was intentional. At the height of their careers, Malcolm’s parents boldly moved their family from a middle-class neighborhood into inner-city Atlanta. Aiming to raise children who understood the complexities of the world around them. That decision and early international experiences in Ghana and Malawi opened Malcolm’s eyes to inequality, social justice, and global responsibility. The wisdom and principles passed down by his parents continue to shape who he is today—on and off the court.
ADVERTISEMENT
Article continues below this ad
Who is Malcolm Brogdon’s Father?
Malcolm Brogdon’s father is Mitchell Gino Brogdon, a respected lawyer and mediator based in Atlanta, Georgia. With a calm demeanor and thoughtful approach to conflict resolution, Mitchell brought more than just legal insight to the Brogdon household; he brought vision.
Mitchell played a critical role in shaping Malcolm’s understanding of the world. One of Mitchell’s most defining decisions as a father was moving the family into inner-city Atlanta. It wasn’t about convenience or prestige but about exposure and empathy. “It was a conscious decision on their part to make sure we grew up with an understanding of what other people had to go through,” Malcolm said.
Mitchell also took young Malcolm to Ghana when he was just 10 years old. There, father and son worked in daycare and maternity facilities. This experience forever changed Malcolm and planted the seeds of his humanitarian focus, especially his commitment to global access to clean water and education. The lessons Mitchell passed on weren’t abstract; they were lived and now ripple out through Malcolm’s work with the Brogdon Family Foundation.
Who is Malcolm Brogdon’s Mother?
Malcolm’s mother, Dr. Jann Adams, is the Associate Vice President at Morehouse College. A historically Black all-male institution with a legacy of developing some of the nation’s greatest civil rights and social justice leaders, including Martin Luther King Jr.. Their alma mater and neighborhood became part of Malcolm’s own daily experience.
ADVERTISEMENT
Article continues below this ad
A dedicated scholar and psychologist, Dr. Adams is more than just an academic…she’s a social advocate. As a follower of Malcolm X, she named her son after the activist and raised him with the same unwavering belief in justice, equity, and dignity. When Malcolm was subjected to racial discrimination in a private school as a child, Dr. Adams didn’t hesitate. She pulled him out, not allowing her son to internalize racism or feel diminished. She taught him self-respect and resistance.
Her influence goes beyond her children. Dr. Adams helped spearhead a social justice and HBCU tour for underserved high school students through the Brogdon Family Foundation. Connecting them with institutions that reflect their history and potential. “Malcolm basically grew up at Morehouse,” she once said. “He literally grew up in Dansby Hall in Morehouse College.” Her leadership and foresight shaped Malcolm into the person he is, and pushes him to strive for more as an athlete.
ADVERTISEMENT
Article continues below this ad
What is Malcolm Brogdon’s Ethnicity?
Malcolm Brogdon is African-American and holds American nationality. His parents, Mitchell Gino Brogdon and Dr. Jann Adams, are African-American and resided in Georgia before their divorce. The Brogdons belong to a family line deeply rooted in civil rights, education, and service. Dating back to Malcolm’s great-grandfather, Eugene Avery Adams Sr., a pastor and early civil rights advocate, and his grandfather, John Hurst Adams, who marched alongside Dr. Martin Luther King Jr.
While it’s impossible not to appreciate Malcolm Brogdon beyond the stat lines, knowing his background makes you respect him even more. His poise isn’t just basketball IQ; it’s lived experience. It’s the product of a powerful upbringing by two parents who didn’t just raise an NBA player…they raised a leader. When Malcolm Brogdon steps on the court, you’re not just watching a basketball player. But the legacy of generations of educators, pastors, activists, and truth-tellers.