ILLINOIS-(MaraviPost)-A devastating accident at Caterpillar’s Mapleton, Illinois, foundry has claimed the life of 39-year-old Steven Dierkes, who tragically fell into a vat of molten iron on his ninth day of employment.
The incident occurred as Dierkes was attempting to collect a sample from the molten metal, but lost his balance and plunged into the 11-foot-deep crucible.
The molten iron, heated to over 2,000 degrees Fahrenheit, instantly incinerated him, leaving behind a grieving family and sparking an investigation into the workplace safety failures that led to his death.
The Occupational Safety and Health Administration (OSHA) investigated the accident and found that the foundry lacked essential safety measures, including guardrails or fall protection systems around the molten iron vats.
OSHA proposed a fine of $145,027 against Caterpillar for these violations, raising questions about whether the penalty is sufficient given the severity of the incident.
Dierkes’ family, including his life partner, Jessica Sutter, and their three daughters, are left to pick up the pieces after his tragic loss.
His obituary described him as a “hard-working teddy bear of a man with calloused hands and a tender heart,” making his untimely death all the more heartbreaking.
The incident highlights the importance of prioritizing workplace safety and ensuring that employers are held accountable for protecting their employees.
As the family seeks justice and answers, the community rallies around them, mourning the loss of a loved one and a valued member of society.
Jan 28 2026 (IPS) – CIVICUS speaks to the Business and Human Rights Centre (BHRC) about labour rights abuses in Myanmar’s garment industry since the 2021 military coup.
Myanmar’s garment sector, which employs hundreds of thousands of workers, is in deep crisis. Since the coup, labour protections have collapsed, independent unions have been dismantled and workers who try to organise face intimidation, dismissal and arrest. Inside factories, reports show multiple cases of child labour, forced overtime, harassment, poverty wages and unsafe conditions. At the same time, rising living costs and US tariffs are pushing many workers further into insecurity as factories close and layoffs become more common. Garment workers, most of them women, are trapped between exploitation, repression and a rapidly shrinking industry.
How have conditions inside Myanmar’s garment factories changed since the coup?
Our monitoring between February 2021 and October 2024 shows a sharp rise in both the number and severity of pre-existing labour rights abuses. Since the coup, factory employers have increasingly worked with the military to restrict organising and silence workers. This collaboration has led to threats, arrests and violent attacks against workers. In one case, security forces carried out joint military and police raids on the homes of workers who demanded unpaid wages and limits on overtime.
Factories have also expanded surveillance. Workers report invasive searches, phone confiscation and installation of CCTV inside factories, including near toilets. Employers also force workers to lie during audits. These practices aim to hide abuses and have exacerbated the abuses workers already faced.
What abuses do garment workers suffer in the workplace?
Factories force workers to meet extreme production targets through excessive and often unpaid overtime. Many workers must stay overnight until dawn, often without enough food, water or ventilation, leading to exhaustion and health problems. Managers threaten and abuse workers who refuse to work overtime or fail to meet targets. We have documented a case where supervisors denied workers food and water as punishment for not meeting targets.
What happen to workers who try to speak out or organise?
Workers who dare speak out face brutal reprisals. After the military declared 16 labour unions and labour rights organisations illegal, arrests, home raids and surveillance increased, particularly against union leaders and activists linked to the Civil Disobedience Movement. The movement began after the coup and brings together workers who refuse to cooperate with military rule through strikes and other forms of non-violent resistance.
Inside factories, employers threaten and dismiss union leaders on false grounds. In one case, a factory reopened and refused to reinstate union members and publicly humiliated them. Employers have also created Workplace Coordination Committees to replace independent unions, denying workers the right to choose their representatives and silencing their complaints. Prominent union leaders such as Myo Myo Aye have been arrested multiple times simply for continuing to organise.
What should international brands be doing in this context?
Under the United Nations Guiding Principles on Business and Human Rights, brands operating in conflict settings must carry out heightened, conflict-sensitive due diligence and demonstrate, with independent and verifiable evidence, that it works. In Myanmar’s current context, where surveillance and violent repression run through all the supply chain, this standard is exceptionally hard to meet.
Any brand that stays must deliver clear and demonstrable improvements in working conditions. Brands that can’t meet this threshold must carry out a responsible exit, working with workers and their representatives and taking steps to reduce harm, rather than adding to the instability garment workers already face under military rule.
Science, research, and scientific discoveries provide solutions to the pressing challenges our society faces and can improve people’s lives. Credit: Shutterstock
URBANA, Illinois, US, Jan 27 2026 (IPS) – Scientists across the U.S., including me, are stressed after a year marked by several changes and challenges, including cuts to science funding that have stalled clinical trials and studies that could improve and save lives. Without funding, scientists worry about how they will support ongoing research and train America’s future workforce, including the next generation of innovators.
These scientific advances have supported agricultural and healthcare advances, expanding U.S. life expectancy by almost 20 years. From vaccines to early disease detection to novel drugs, the returns on funding science are substantial.
We need science. Moments like the challenges of today call for reflection and offer opportunities to readjust, evolve, and move forward, including finding new ways to engage with the public and policymakers and to fund and conduct science creatively
Science, research, and scientific discoveries, after all, provide solutions to the pressing challenges our society faces and can improve people’s lives. Science guides us through these challenges, inspires us, and unites many curious minds.
We need science. Moments like the challenges of today call for reflection and offer opportunities to readjust, evolve, and move forward, including finding new ways to engage with the public and policymakers and to fund and conduct science creatively.
So how do we adjust? What actions can scientists take now?
First, scientists need to keep showing up and find creative ways to communicate science and the solutions being generated to the public, policymakers, and government administrators.
This includes unpacking how science solutions address the issues everyday people face, including their economic future, and how science advancements align with the challenges people face now.
Communicating science and research outcomes to the broader public, policymakers, and other stakeholders in the science enterprise is not easy. However, scientists have continued to develop creativeways to improve how we communicate science. Specifically, scientists are using multiple formats, including storytelling, infographics, animations, and interactive games and graphics.
These efforts must continue to expand, tapping into the many available ways to communicate science, including podcasts, blogs, social media, radio, TV, and op-eds.
To ensure maximum participation by scientists, universities and research institutions should find innovative ways to incentivize students and scientists to engage with the public and share their research.
Complementing these efforts, universities and research institutions, along with professional societies to which scientists belong, can continue to offer workshops and training to help scientists become better communicators.
For example, between 2008 and 2022, the American Association for the Advancement of Science offered several science communication workshops.
Alongside these efforts, professional societies have also recognized elected officials who have continued to champion the role of science in addressing persistent societal challenges. For example, in 2025, ESA recognized Senator Susan Collins of Maine as the society’s 2025 Champion of Entomology for her continued support for science and research funding and for introducing several bills that are still pending Senate and House votes.
Second, we need to continue strengthening public and policymakers’ trust in science by improving peer review processes and ensuring that science remains transparent, rigorous, and repeatable, and that the credibility of published science remains intact. In recent years, there has been a rapidincrease in the number of paper mills producing fraudulent scientific papers. These science integrity challenges undermine scientific enterprises and create distrust among the public.
Strengthening public trust in science and scientists can take many forms, including convening town halls and public forums. Other creative ways include involving the public in citizen science research and fieldwork, allowing the public to be involved from the outset, including building the research project goals and a compelling justification for why the research question being addressed is important.
Engaging the public and involving them in shaping the scientific questions scientists pursue can not only strengthen public trust in science but also enrich outcomes by incorporating local or experiential knowledge. In doing so, public engagement helps ensure that the solutions generated by these shared projects address and solve challenges that are grounded, relevant, and meaningful to communities and the public we aim to serve.
For example, in my research on plant-microbe-insect interactions, which aims to help feed a growing population sustainably amid changing environments and to strengthen plant resilience against biotic and abiotic stressors such as insects, drought, and flooding, collaborating with farmers can directly shape the pests and crops I study and guide the questions I pursue. By doing so, the resulting research insights become responsive to the current agricultural challenges American farmers face.
Thirdand most importantly, there is an urgent need to develop a long-term vision and establish unbreakable funding frameworks for science to ensure that the gains we have made so far are preserved. Scientists, national academies of science, government administrators, elected officials, policymakers, the military, industry, NGOs, the public, think tanks, foundations, and all stakeholders in the science enterprise must work together to chart a new path forward.
Without bending back too far, scientists can stop, reflect, and find their path forward.
It is necessary to bring together all stakeholders in the science enterprise to create new science funding frameworks that are both acceptable and reasonable. Otherwise, the value of science and research, along with the gains made to date, could be lost.
It’s time for scientists to extend the olive branch, redouble our efforts to communicate science to society, and chart a path forward that brings everyone on board.
Esther Ngumbi, PhD is Assistant Professor, Department of Entomology, African American Studies Department, University of Illinois at Urbana-Champaign
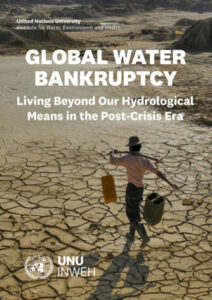
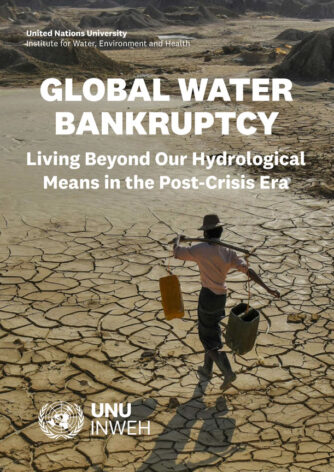
Flagship report calls for fundamental reset of global water agenda as irreversible damage pushes many basins beyond recovery.
UNITED NATIONS, Jan 21 2026 (IPS) – The world is already in the state of “water bankruptcy”. In many basins and aquifers, long-term overuse and degradation mean that past hydrological and ecological baselines cannot realistically be restored.
While not every basin or country is water-bankrupt, enough critical systems around the world have crossed these thresholds, and are interconnected through trade, migration, climate feedbacks, and geopolitical dependencies, that the global risk landscape is now fundamentally altered.
The familiar language of “water stress” and “water crisis” is no longer adequate. Stress describes high pressure that is still reversible. Crisis describes acute, time-bound shocks. Water bankruptcy must be recognized as a distinct post-crisis state, where accumulated damage and overshoot have undermined the system’s capacity to recover.
A group of women fetching water from a dam in Taha, Northern Region of Ghana. Credit: Evans Ahorsu. Source: UN University’s Institute for Water, Environment and Health
Water bankruptcy management must address insolvency and irreversibility. Unlike financial bankruptcy management, which deals only with insolvency, managing water bankruptcy is concerned with rebalancing demand and supply under conditions where returning to baseline conditions is no longer possible.
Anthropogenic drought is central to the world’s new water reality. Drought and water shortage are increasingly driven by human activities, over-allocation, groundwater depletion, land and soil degradation, deforestation, pollution, and climate change, rather than natural variability alone. Water bankruptcy is the outcome of long-term anthropogenic drought, not just bad luck with hydrological anomalies.
Water bankruptcy is about both quantity and quality. Declining stocks, polluted rivers, and degrading aquifers, and salinized soils mean that the truly usable fraction of available water is shrinking, even where total volumes may appear stable.
Managing water bankruptcy requires a shift from crisis management to bankruptcy management. The priority is no longer to “get back to normal”, but to prevent further irreversible damage, rebalance rights and claims within degraded carrying capacities, transform water-intensive sectors and development models, and support just transitions for those most affected.
Governance institutions must protect both water and its underlying natural capital. The existing institutions focus on protecting water as a good or service disregarding the natural capital that makes water available in the first place. Efforts to protect a product are ineffective when the processes that produce it are disrupted.
Recognizing water bankruptcy calls for developing legal and governance institutions that can effectively protect not only water but also the hydrological cycle and natural capital that make its production possible.
Water bankruptcy is a justice and security issue. The costs of overshoot and irreversibility fall disproportionately on smallholder farmers, rural and Indigenous communities, informal urban residents, women, youth, and downstream users, while benefits have often accrued to more powerful actors. How societies manage water bankruptcy will shape social cohesion, political stability, and peace.
Water bankruptcy management combines mitigation with adaptation. While water crisis management paradigms seek to return the system to normal conditions through mitigation efforts only, water bankruptcy management focuses on restoring what is possible and preventing further damages through mitigation combined with adaptation to new normals and constraints.
Water can serve as a bridge in a fragmented world. Water can align national priorities with international priorities and improve cooperation between and within nations. Roughly 70% of global freshwater withdrawals are used for agriculture, much of it by farmers in the Global South. Elevating water in global policy debates can help rebuild trust between South and North but also within nations, between rural and urban, left and right constituencies.
Water must be recognized as an upstream sector. Most national and international policy agendas treat water as a downstream impact sector where investments are focused on mitigating the imposed problems and externalities. The world must recognize water as an upstream opportunity sector where investments have long-term benefits for peace, stability, security, equity, economy, health, and the environment.
Water is an effective medium to fulfill the global environmental agenda. Investments in addressing water bankruptcy deliver major co-benefits for the global efforts to address its environmental problems while addressing the national security concerns of the UN member states.
Elevating water in the global policy agenda can renew international cooperation, increase the efficiency of environmental investments, and reaccelerate the halted progress of the three Rio Conventions to address climate change, biodiversity loss, and desertification.
A new global water agenda is urgently needed. Existing agendas and conventional water policies, focused mainly on WASH, incremental efficiency gains and generic IWRM guidelines, are not sufficient for the world’s current water reality. A fresh water agenda must be developed that takes Global Water Bankruptcy as a starting point and uses the 2026 and 2028 UN Water Conferences, the conclusion of the Water Action Decade in 2028, and the 2030 SDG 6 timeline as milestones for resetting how the world understands and governs water.
Global Water Bankruptcy: Living Beyond Our Hydrological Means in the Post-Crisis Era | UN University Institute for Water, Environment and Health (UNU-INWEH) (20 January) (press release)
Support Paper Madani K. (2026) Water Bankruptcy: The Formal Definition, Water Resources Management, 40 (78) doi: 10.1007/s11269-025-04484-0)
Cardiologist Dr. Marwan Sultan, then Director of the Indonesian Hospital in north Gaza, in February 2025 showing damage to hospital equipment following an Israeli attack on the facility a few months prior. In July 2025, Dr. Sultan was killed in an Israeli strike on the apartment where he was sheltering with his family. Credit: PHR/GHRC
BRATISLAVA, Jan 14 2026 (IPS) – Israel must lift all restrictions on medicine, food and aid coming into Gaza, rights groups have demanded, as two reports released today (Jan 14) document how maternal and reproductive healthcare have been all but destroyed in the country.
The reports from the two groups, which are independent organizations, provide both detailed clinical analysis of the collapse of Gaza’s health system and its medical consequences as well as firsthand testimonies from clinicians and pregnant and breastfeeding women in Gaza forced to live and care for their newborns in extreme conditions.
And the organizations say that with conditions improving only marginally for many women despite the current ceasefire, Israel must roll back restrictions placed on aid and immediately help ensure people in Gaza get access to the healthcare they need.
“Israel’s destruction of Gaza’s health infrastructure, combined with untreated malnutrition resulting from restrictions on food and medical supplies, including baby formula, has created an environment in which the fundamental biological processes of reproduction and survival have been systematically destroyed, resulting in known and foreseeable harm, pain, suffering, and death,” Sam Zarifi, Physicians for Human Rights (PHR) Executive Director, said.
“Israel must immediately allow food and essential medical material to enter Gaza with a proper medical plan for helping the besieged population,” he added.
Israeli military operations following Hamas’s attack on Israel on October 7, 2023, have left massive destruction across Gaza, including to healthcare facilities. According to UNICEF, 94 percent of hospitals have been damaged or destroyed.
Destroyed incubators and equipment at the Kamal Adwan Hospital Neonatal Intensive Care Unit in north Gaza, following the targeting and raid of the facility by the Israeli forces in December 2024. Credit: PHR/GHRC
Maternal and reproductive healthcare has suffered. Before the war, Gaza had eight neonatal intensive care units with 178 incubators. Today, the number of incubators has dropped by 70 percent. In the north, there were 105 incubators across three NICUs, now there are barely any functional units remaining, UNICEF told IPS.
It says that the numbers of low birth weight babies have nearly tripled compared to pre-war levels and the number of first-day deaths of babies increased by 75 percent.
The PHR and PHR-I reports paint a similar picture.
The PHR report, which focuses on the period between January 2025 and October 2025 when a ceasefire was agreed, details how between May and June last year, the Palestinian Ministry of Health reported a 41 percent decrease in the birth rate in Gaza compared to the same time period in 2022; there was a significant increase in miscarriages that affected more than 2,600 women, and 220 pregnancy-related deaths that occurred before delivery.
The ministry also reported a sharp increase in premature births and low birth weight cases; over 1,460 babies were reported to be born prematurely, while more than 2,500 were admitted to neonatal intensive care. Newborn deaths also increased, with at least 21 babies reported to have died on their first day of life.
Meanwhile, the PHR-I report includes personal testimonies illustrating the severe problems pregnant women and women with newborns have faced in Gaza during the war, from lacking safe routes to care and being forced to give birth in unsanitary, dangerous conditions to battling hunger and severe food shortages as they try to breastfeed their children.
One woman, Samah Muhammad Abu Mustafa, a 30-year-old mother of two from Khuza’a, Khan Youni, described how when her contractions began in the middle of the night, because there were no vehicles and very few ambulances, which are reserved for shelling or other critical emergencies, she had to walk a long distance through rain. When she eventually reached the hospital, she said it was “horrifying.”
“I swear, one woman gave birth in the corridor, and her baby died. It was very crowded, and the doctors worked nonstop. I felt as though I could give birth at any moment. After giving birth to my eldest daughter, I was told I should not deliver naturally again because my pelvis was too narrow. Despite this, the doctors said I would have to deliver naturally because a cesarean section required anesthesia, and there was not enough available. I stood for three hours until it was finally my turn, without sitting even for a moment,” she said.
But despite the October 2025 ceasefire, massive problems remain with women’s access to and the provision of, maternal and reproductive healthcare in Gaza.
“Maternal health units in Gaza are largely non-functional and face critical shortages of essential medicines, consumables, and equipment,” Lama Bakri, project coordinator in the Occupied Territories Department at PHR-I, told IPS.
“Neonatal and diagnostic equipment remains scarce or blocked, including portable incubators for premature and low-birth-weight newborns. Although some aid has entered since the ceasefire, these gaps are not being addressed at the scale required, and meaningful improvement in the immediate future remains unlikely.”
Malnutrition also remains a serious problem.
“The ceasefire has allowed us to significantly scale up our nutrition response, but we are still treating pregnant and breastfeeding women for acute malnutrition in alarmingly high numbers,” Ricardo Pires, Communication Manager, Division of Global Communications & Advocacy at UNICEF, told IPS.
He said that between July and September 2025 about 38 percent of pregnant women screened were diagnosed with acute malnutrition.
“In October alone, we admitted 8,300 pregnant and breastfeeding women for treatment, about 270 a day, in a place where there was no discernible malnutrition among this group before October 2023,” he added.
UNICEF has documented almost 6,800 children admitted for acute malnutrition treatment in November 2025 compared to 4,700 cases in November 2024. So far, the number of admitted cases more than doubled in 2025 compared to 2024: almost 89,000 admissions of children to date in 2025, compared to 40,000 cases in 2024, and almost none before 2023.
“What we’re seeing is that no child meets minimum dietary diversity standards, and two-thirds of children are surviving on just two food groups or less. Around 90 percent of caregivers reported their children had been sick in the previous two weeks, which compounds the malnutrition crisis,” Pires said.
And there are fears for the longer-term demographic future of Gaza given the damage to maternal and reproductive healthcare.
“For Gaza’s demographic future, the implications are serious. Even with reconstruction, we will be dealing with a generation of children who were scarred before they took their first breath, children who may face lifelong health complications, developmental challenges, and the effects of stunting. The rebuilding must start now, but we should be clear-eyed: the damage to maternal and newborn health will echo for years, potentially decades,” said Pires.
But others say that with cooperation between international actors and the right political will, the situation need not remain so dire.
“To rehabilitate the population after everything that has happened is going to be a real issue, [but] now there is a Board of Peace, the needs of pregnant women and maternal and reproductive healthcare can be prioritized,” Zarifi told IPS.
“The capacity and the will exist among Gazans and Gazan healthcare workers to rebuild the healthcare system, including maternal and reproductive health services,” added Bakri. “The primary obstacle is not technical or professional but political: Israel’s control over Gaza’s borders and the restrictions on the entry of essential equipment, medical supplies, and reconstruction materials. With unrestricted access to what is needed to rehabilitate hospitals, rebuild destroyed units, and restock essential medicines, recovery is entirely feasible. Whether maternal and reproductive healthcare can return to pre-war levels depends on sustained international pressure to allow that access.”
Although some aid has entered since the ceasefire, these gaps are not being addressed at the scale required, and meaningful improvement in the immediate future remains unlikely.
However, while both NGOs like PHR and PHR-I and others, alongside international bodies like the UN, stress that any recovery and reconstruction in Gaza requires the ceasefire to hold and consolidate, repeated violations underline its fragility, and the effect that has on women.
Meanwhile, PHR and PHR-I point out that extreme weather and ongoing Israeli restrictions on medicine and food getting to Gaza to this day continue to severely affect pregnant women, new mothers, and babies. On top of this, Israel has also announced it will bar 37 international aid groups from working in Gaza, potentially compounding the problems.
Bakri said such measures were jeopardizing what small gains had been made since the ceasefire and “raise serious concerns about whether the situation can improve.”
“Even after the ceasefire, while bombardment has decreased, the reality these women face remains catastrophic – not only for their bodies and well-being but for the survival of the entire society,” said Bakri.
Zarifi added, “We are worried that the restrictions placed by Israel on some of the major actors in the humanitarian response will hamper access to assistance for those that need it. We have raised questions with the Israeli government as to why specific medicines are not allowed to be brought into Gaza and they say that they are not stopping them from being brought in but they can be brought in by commercial means. That is hard for people who can barely put any money together. These medicines should definitely be coming in through humanitarian channels.”
He also highlighted how important the issue of accountability is in ensuring any progress is made in rebuilding healthcare in Gaza and also limiting the probability of similar devastation in the future.
Both reports concluded that the harms caused by Israeli attacks are not isolated incidents but part of an ongoing pattern of systematic damage to the health of women and their children in Gaza, amounting to reproductive violence.
Israel has denied this and said that attacks on hospitals in Gaza have been because the medical facilities are being used by Hamas, and it has maintained that its forces adhere to international law.
While under international law healthcare facilities have special protection even in war, and attacks on them are prohibited, that protection is lost if they are deemed to fulfill criteria to be considered military objectives, such as housing militaries and arms.
However, any attack on them must still comply with the fundamental principles of distinction, proportionality and precautions in attack and failure to respect any of these principles constitutes a breach of international humanitarian law, according to the UN.
“These attacks are part of a deliberate policy designed to create a domino effect of suffering. From starvation and militarized aid distribution by the GHF, to lack of access to clean water, repeated displacement orders, living in shelters under continuous bombardment, and exposure to infections, disease, and harsh weather, the attacks on maternal and reproductive healthcare are another piece of this puzzle. Together, these conditions were created to systematically destroy the fabric of life in Gaza and reduce the population’s ability to survive,” said Bakri.
“The Israeli government has justified attacks on healthcare facilities by saying this was a problem caused by Hamas. We haven’t had an indication of this but it might be true. But in any case there has to be an investigation of these incidents and we hope the Israeli government will carry out such an investigation,” said Zarifi.
“But what is really alarming to us is that the norms prohibiting attacks on healthcare have been repeatedly violated, and there are also laws governing the protection of women and children that appear to have been violated. The only thing that makes these norms work is accountability. There has to be accountability for what happened, as it is the only way we can ensure that what has happened won’t happen in other conflicts. Impunity is watched by other actors around the world,” he added.
WASHINGTON, DC – NOVEMBER 14: U.S. Speaker of the House Mike Johnson (R-LA) speaks during a news conference after a weekly Republican conference meetingin the U.S. Capitol Building on November 14, 2023 in Washington, DC. During the news conference House Republican leadership spoke to reporters about a range of topics including the upcoming vote on a continuing resolution to fund the government through early 2024. (Photo by Anna Moneymaker/Getty Images)
Minnesota state law enforcement officials are working with the FBI to investigate the fatal shooting of a Minneapolis woman by an Immigrations and Customs Enforcement officer. U.S. forces boarded a tanker carrying sanctioned oil after a two-week chase across the Atlantic, as the Trump administration expands plans to take control of Venezuela’s oil sales indefinitely. And Health Secretary Robert F. Kennedy Jr.’s new dietary guidelines flip decades of advice, elevating meat and dairy and alarming many public health researchers.
Want more analysis of the most important news of the day, plus a little fun? Subscribe to the Up First newsletter.
Today’s episode of Up First was edited by Rebekah Metzler, Kelsey Snell, Kate Bartlett, Mohamad ElBardicy, and Alice Woelfle.
It was produced by Ziad Buchh, Nia Dumas and Christopher Thomas.
We get engineering support from David Greenburg. Our technical director is Stacey Abbott.
And our deputy Executive Producer is Kelley Dickens.




 Myanmar’s garment sector, which employs hundreds of thousands of workers, is in deep crisis. Since the coup, labour protections have collapsed, independent unions have been dismantled and workers who try to organise face intimidation, dismissal and arrest. Inside factories, reports show multiple cases of child labour, forced overtime, harassment, poverty wages and unsafe conditions. At the same time, rising living costs and US tariffs are pushing many workers further into insecurity as factories close and layoffs become more common. Garment workers, most of them women, are trapped between exploitation, repression and a rapidly shrinking industry.
Myanmar’s garment sector, which employs hundreds of thousands of workers, is in deep crisis. Since the coup, labour protections have collapsed, independent unions have been dismantled and workers who try to organise face intimidation, dismissal and arrest. Inside factories, reports show multiple cases of child labour, forced overtime, harassment, poverty wages and unsafe conditions. At the same time, rising living costs and US tariffs are pushing many workers further into insecurity as factories close and layoffs become more common. Garment workers, most of them women, are trapped between exploitation, repression and a rapidly shrinking industry.